Capsoni Nicolò, Azin Giulia Maria, Scarnera Marida, Bettina Marco, Breviario Riccardo, Ferrari Laura, Ferrari Camilla, Privitera Daniele, Vismara Chiara, Bielli Alessandra, Galbiati Filippo, Bernasconi Davide Paolo, Merli Marco, Bombelli Michele
School of Medicine and Surgery, University of Milan-Bicocca, Milan, Italy.
Department of Emergency Medicine, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy.
Intern Emerg Med. 2025 Mar;20(2):573-583. doi: 10.1007/s11739-024-03692-7. Epub 2024 Jul 13.
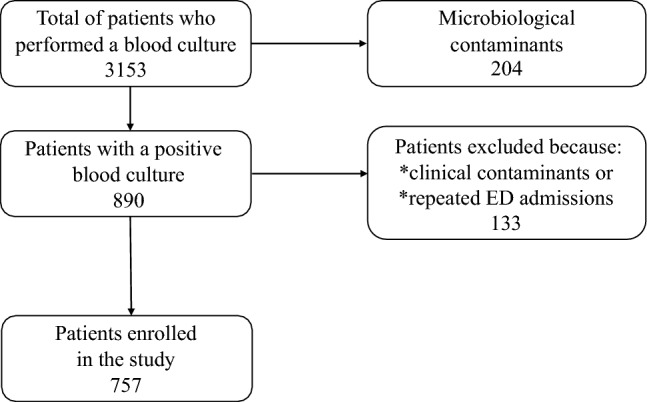
Multidrug-resistant organisms (MDROs) are prevalent in patients admitted to the Emergency Department (ED) and increase the risk of inappropriate empirical antibiotic therapy. Risk stratification for MDRO infection is essential to early identify patients requiring empirical broad-spectrum antibiotic therapy, but it remains challenging for emergency physicians. This study aimed to evaluate prevalence, risk factors, and outcomes of patients admitted to the ED with a bloodstream infection (BSI) caused by MDROs. A retrospective observational study enrolling all consecutive adult patients admitted with a BSI to the ED of Niguarda Hospital, Italy, from January 2019 to December 2021 was performed. 757 patients were enrolled, 14.1% with septic shock. 156 (20%) patients had a BSI caused by MDRO: extended-spectrum beta-lactamase (ESBL) producing Enterobacterales were the most prevalent followed by methicillin-resistant Staphylococcus aureus (MRSA). Risk factors for BSI due to MDRO and specifically for ESBL were chronic renal failure (OR 2.2; 95%CI 1.4-3.6), nursing home residency (OR 4.4; 95%CI 1.9-10.2) and antibiotic therapy in the last 90-days (OR 2.6; 95%CI 1.7-4), whereas for MRSA were dialysis (OR 12.3; 95%CI 1.8-83), antibiotic therapy and/or hospital admission in the past 90-days (OR 3.6; 95%CI 1.2-10.6) and ureteral stent or nephrostomy (OR 7.8; 95%CI 1.5-40.9). Patients with BSI due to MDRO had a higher rate of inappropriate empirical antibiotic therapy (50%) and longer length of stay, but no higher in-hospital mortality. Among patients admitted to the ED with a BSI, MDROs are frequent and often associated with inappropriate empirical antibiotic therapy. Specific updated risk factors for MDRO may help clinicians to better identify patients requiring a broader antibiotic therapy in the ED, while awaiting microbiological results.
多重耐药菌(MDROs)在急诊科(ED)收治的患者中普遍存在,并增加了不适当经验性抗生素治疗的风险。MDRO感染的风险分层对于早期识别需要经验性广谱抗生素治疗的患者至关重要,但对急诊科医生来说仍然具有挑战性。本研究旨在评估因MDROs导致血流感染(BSI)而入住急诊科的患者的患病率、危险因素和结局。对2019年1月至2021年12月期间意大利尼瓜尔达医院急诊科收治的所有连续成年BSI患者进行了一项回顾性观察研究。共纳入757例患者,其中14.1%患有感染性休克。156例(20%)患者的BSI由MDROs引起:产超广谱β-内酰胺酶(ESBL)的肠杆菌科细菌最为常见,其次是耐甲氧西林金黄色葡萄球菌(MRSA)。MDROs导致BSI的危险因素,特别是ESBL的危险因素为慢性肾衰竭(比值比[OR]2.2;95%置信区间[CI]1.4 - 3.6)、居住在养老院(OR 4.4;95%CI 1.9 - 10.2)以及过去90天内接受抗生素治疗(OR 2.6;95%CI 1.7 - ),而MRSA的危险因素为透析(OR 12.3;95%CI 1.8 - 83)、过去90天内接受抗生素治疗和/或住院(OR 3.6;95%CI 1.2 - 10.6)以及输尿管支架或肾造瘘术(OR 7.8;95%CI 1.5 - 40.9)。因MDROs导致BSI的患者不适当经验性抗生素治疗的发生率较高(50%)且住院时间较长,但院内死亡率没有更高。在因BSI入住急诊科的患者中,MDROs很常见,且常常与不适当的经验性抗生素治疗相关。MDROs的特定更新危险因素可能有助于临床医生在等待微生物学结果时,更好地识别急诊科中需要更广泛抗生素治疗的患者。