Dosanjh Amandeep, Coupland Benjamin, Mytton Jemma, King Dominic Stephen, Mintz Harriet, Lock Anna, Nanton Veronica, Mariappan Param, Trudgill Nigel, Patel Prashant
University of Birmingham Institute of Cancer and Genomic Sciences, Birmingham, UK.
Research and Development, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
BMJ Support Palliat Care. 2024 Jul 13;14(e2). doi: 10.1136/spcare-2024-004937.
To assess the outcomes of percutaneous nephrostomy in England for renal decompression, in the context of metastatic cancer.
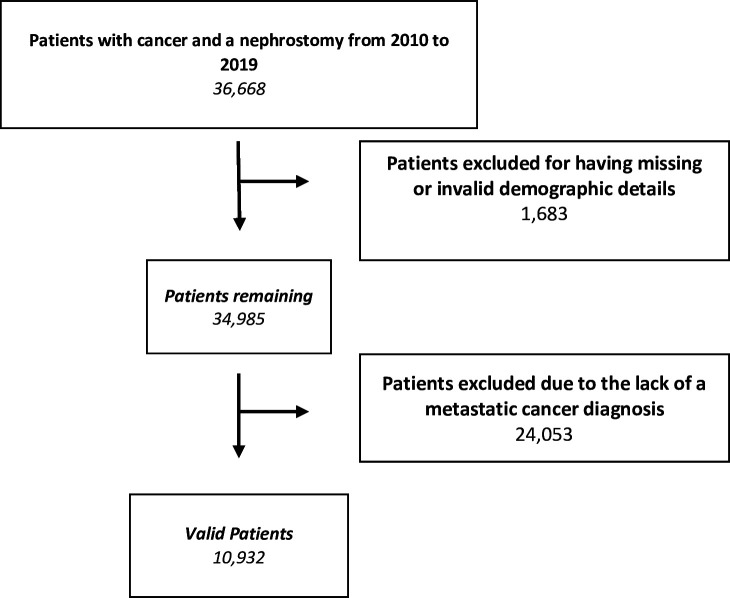
Retrospective observational study of all patients undergoing nephrostomy with a diagnosis of metastatic cancer from 2010 to 2019 in England, identified and followed up within Hospital Episode Statistics.The primary outcome measure was mortality (14-day and 30-day postprocedure). Secondary outcomes included subsequent chemotherapy or surgery and direct complications of nephrostomy.
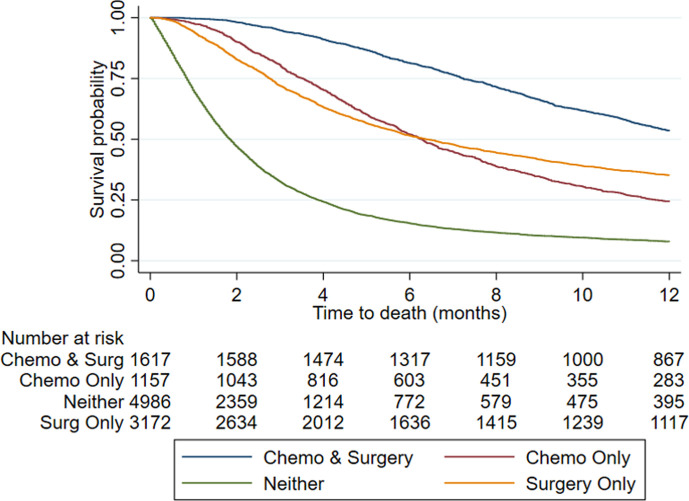
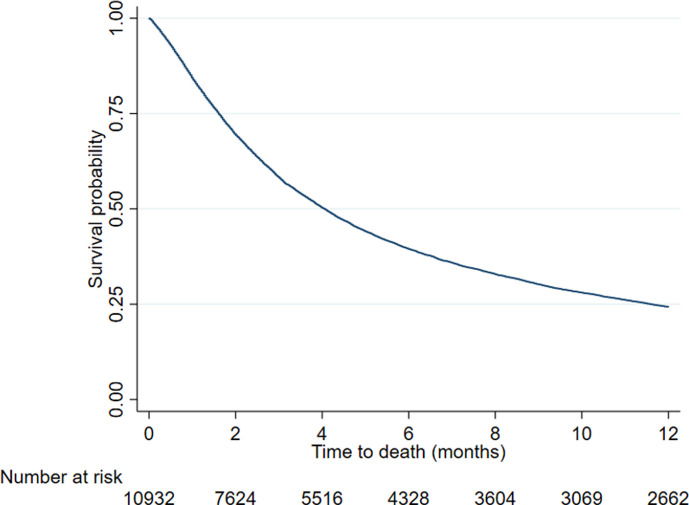
10 932 patients were identified: 58.0% were male, 51.0% were >70 years old and 57.7% had no relevant comorbidities (according to Charlson's criteria, other than cancer).1 in 15 patients died within 14 days of nephrostomy and 1 in 6 died within 30 days. Factors associated with higher 30-day mortality were the presence of comorbidities (Charlson score 1-4 (OR 1.27, 95% CI 1.08 to 1.50, p=0.003), score 5+ (OR 1.29, 95% CI 1.14 to 1.45), p<0.001)); inpatient nephrostomy (OR 3.76, 95% CI 2.75 to 5.14, p<0.001) and admitted under the care of specialities of internal medicine (OR 2.10, 95% CI 1.84 to 2.40, p<0.001), oncology (OR 1.80, 95% CI 1.51 to 2.15, p<0.001), gynaecology/gynaeoncology (OR 1.66, 95% CI 1.21 to 2.28, p=0.002) or general surgery (OR 1.62, 95% CI 1.32 to 1.98, p<0.001)), compared with urology.25.4% received subsequent chemotherapy. Receiving chemotherapy was associated with younger patients (eg, age 18-29 (OR 4.04, 95% CI 2.66 to 6.12, p<0.001) and age 30-39 (OR 3.07, 95% CI 2.37 to 3.97, p<0.001)) and under the care of oncology (OR 1.60, 95% CI 1.40 to 1.83, p<0.001) or gynaecology/gynaeoncology (OR 1.64, 95%CI 1.28 to 2.10, p<0.001) compared with urology.43.8% had subsequent abdominopelvic surgery. Not receiving surgery was associated with inpatient nephrostomy (OR 0.82, 95%CI 0.72 to 0.95,p=0.007): non-genitourinary cancers (eg, gynaecology/gynaeoncology cancer (OR 0.86, 95% CI 0.74 to 0.99, p=0.037)); and under the care of a non-surgical specialty (medicine (OR 0.69, 95% CI 0.63 to 0.77, p<0.001), oncology (OR 0.58, 95% CI 0.51 to 0.66, p<0.001)).24.5% of patients had at least one direct complication of nephrostomy: 12.5% required early exchange of nephrostomy, 8.1% had bleeding and 6.7% had pyelonephritis.
The decision to undertake nephrostomy in patients with poor prognosis cancer is complex and should be undertaken in a multidisciplinary team setting. Complication rates are high and minimal survival benefit is derived in many patients, especially in the context of emergency inpatient care.
在转移性癌症背景下,评估英格兰经皮肾造瘘术用于肾脏减压的效果。
对2010年至2019年在英格兰接受肾造瘘术且诊断为转移性癌症的所有患者进行回顾性观察研究,通过医院事件统计数据进行识别和随访。主要结局指标为死亡率(术后14天和30天)。次要结局包括后续化疗或手术以及肾造瘘术的直接并发症。
共识别出10932例患者:58.0%为男性,51.0%年龄大于70岁,57.7%无相关合并症(根据查尔森标准,不包括癌症)。15例患者中有1例在肾造瘘术后14天内死亡,6例中有1例在30天内死亡。与30天死亡率较高相关的因素包括存在合并症(查尔森评分1 - 4(比值比1.27,95%置信区间1.08至1.50,p = 0.003),评分5 +(比值比1.29,95%置信区间1.14至1.45,p < 0.001));住院肾造瘘术(比值比3.76,95%置信区间2.75至5.14,p < 0.001)以及在内科(比值比2.10,95%置信区间1.84至2.40,p < 0.001)、肿瘤学(比值比1.80,95%置信区间1.51至2.15,p < 0.001)、妇科/妇科肿瘤学(比值比1.66,95%置信区间1.21至2.28,p = 0.002)或普通外科(比值比1.62,95%置信区间1.32至1.98,p < 0.001)专科护理下入院,与泌尿外科相比。25.4%的患者接受了后续化疗。接受化疗与较年轻患者相关(例如,年龄18 - 29岁(比值比4.04,95%置信区间2.66至6.12,p < 0.001)和年龄30 - 39岁(比值比3.07,95%置信区间2.37至3.97,p < 0.001))以及在肿瘤学(比值比1.60,95%置信区间1.40至1.83,p < 0.001)或妇科/妇科肿瘤学(比值比1.64,95%置信区间1.28至2.10,p < 0.001)专科护理下,与泌尿外科相比。43.8%的患者接受了后续腹部盆腔手术。未接受手术与住院肾造瘘术相关(比值比0.82,95%置信区间0.72至0.95,p = 0.007):非泌尿生殖系统癌症(例如,妇科/妇科肿瘤学癌症(比值比0.86,95%置信区间0.74至0.99,p = 0.037));以及在非手术专科护理下(内科(比值比0.69,95%置信区间0.63至0.77,p < 0.001),肿瘤学(比值比0.58,95%置信区间0.51至0.66,p < 0.001))。24.5%的患者至少发生了一种肾造瘘术的直接并发症:12.5%需要早期更换肾造瘘管,8.1%有出血,6.7%有肾盂肾炎。
对预后不良的癌症患者进行肾造瘘术的决策很复杂,应在多学科团队环境中进行。并发症发生率很高,许多患者生存获益极小,尤其是在急诊住院治疗的情况下。