School of Laboratory Medicine, Chengdu Medical College, Chengdu, 610500, China.
Department of Nephrology, Jinniu Hospital, Sichuan Provincial People's Hospital, Jinniu People's Hospital, Chengdu, 610072, China.
Nutr J. 2024 Jul 15;23(1):75. doi: 10.1186/s12937-024-00980-y.
An increasing number of studies shown that inadequate energy intake causes an increase in adverse incidents in chronic kidney disease (CKD) patients on low-protein diets (LPD). The study aimed to investigate the relationship between energy intake and cardiovascular mortality in CKD patients on a LPD.
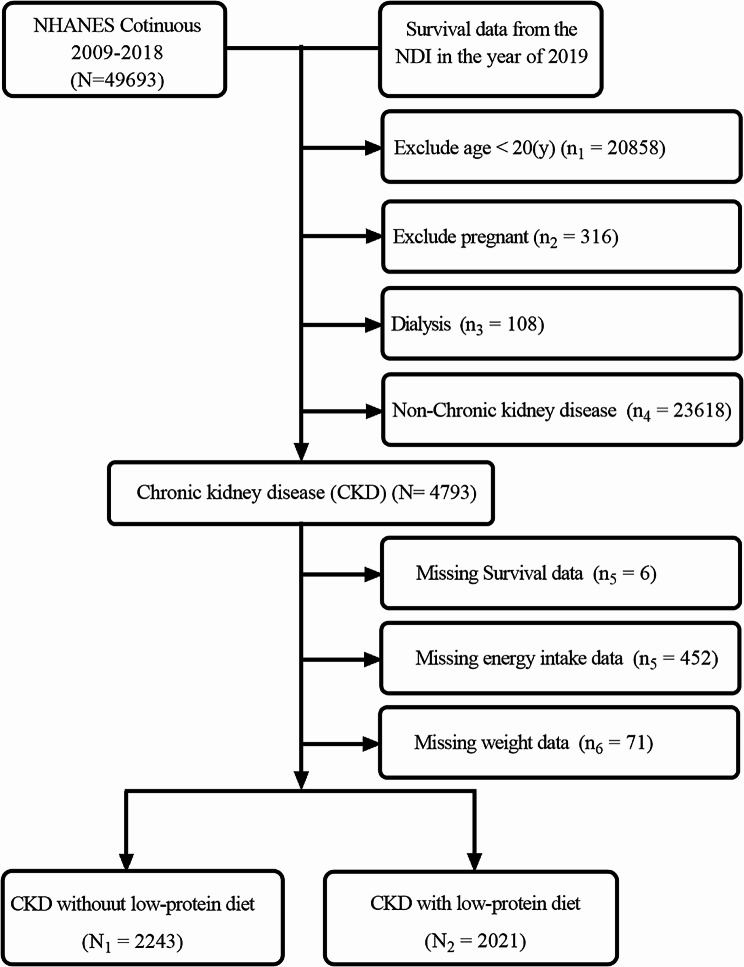
This was a cross-sectional study, a total of 4264 CKD patients were enrolled from the NHANES database between 2009 and 2018. Restricted cubic spline plots and Cox regression analysis were used to analyze the association between energy intake and cardiovascular mortality in CKD patients on a LPD. Additionally, a nomogram was constructed to estimate cardiovascular survival in CKD patients on a LPD.
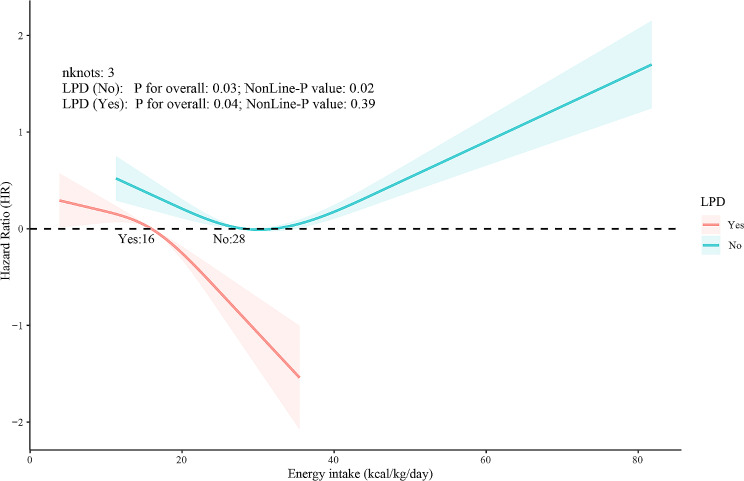
Among CKD patients on a LPD in the United States, 90.05% had an energy intake of less than 25 kcal/kg/day, compared to 36.94% in CKD patients on a non-LPD. Energy intake and cardiovascular mortality showed a linear relationship in CKD patients on a LPD, while a 'U-shaped' relationship was observed in CKD patients on a non-LPD. Multifactorial Cox regression models revealed that for Per-standard deviation (Per-SD) decrement in energy intake, the risk of cardiovascular mortality increased by 41% (HR: 1.41, 95% CI: 1.12, 1.77; P = 0.004) in CKD patients on a LPD. The concordance index of the nomogram was 0.79 (95% CI, 0.75, 0.83).
CKD patients, especially those on a LPD, have significantly inadequate energy intake. Lower energy intake is associated with higher cardiovascular mortality in CKD patients on a LPD.
越来越多的研究表明,能量摄入不足会增加接受低蛋白饮食(LPD)治疗的慢性肾脏病(CKD)患者的不良事件发生率。本研究旨在探讨 LPD 治疗的 CKD 患者能量摄入与心血管死亡率之间的关系。
这是一项横断面研究,共纳入了 2009 年至 2018 年 NHANES 数据库中的 4264 例 CKD 患者。采用受限立方样条图和 Cox 回归分析来分析 LPD 治疗的 CKD 患者能量摄入与心血管死亡率之间的关系。此外,还构建了一个列线图来估计 LPD 治疗的 CKD 患者的心血管生存情况。
在美国接受 LPD 治疗的 CKD 患者中,有 90.05%的患者能量摄入低于 25 kcal/kg/天,而接受非 LPD 治疗的 CKD 患者中这一比例为 36.94%。LPD 治疗的 CKD 患者中,能量摄入与心血管死亡率呈线性关系,而非 LPD 治疗的 CKD 患者中则呈“U 型”关系。多因素 Cox 回归模型显示,对于 LPD 治疗的 CKD 患者,每标准偏差(Per-SD)的能量摄入减少,心血管死亡率的风险增加 41%(HR:1.41,95%CI:1.12,1.77;P=0.004)。列线图的一致性指数为 0.79(95%CI,0.75,0.83)。
CKD 患者,尤其是接受 LPD 治疗的患者,能量摄入明显不足。较低的能量摄入与 LPD 治疗的 CKD 患者心血管死亡率升高有关。