Gresnigt F M J, Heikamp L K, van Essen J J W, Walraven L F J, van Ofwegen-Hanekamp C E E, Mollink S, Franssen E J F, de Lange D W, Riezebos R K
Emergency Department, OLVG Hospital, Oosterpark 9, Amsterdam 1091 AC, the Netherlands.
Dutch Poison Information Center (DPIC), UMC Utrecht, University Utrecht, Utrecht 3508 GA, the Netherlands.
Toxicol Rep. 2024 Jun 18;13:101680. doi: 10.1016/j.toxrep.2024.05.010. eCollection 2024 Dec.
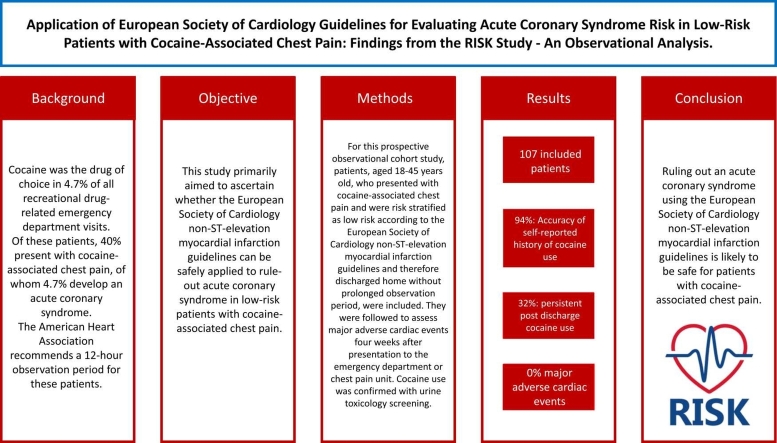
Cocaine was the drug of choice in 4.7 % of all recreational drug-related emergency department visits. Of these patients, 40 % present with cocaine-associated chest pain, of whom 4.7 % develop an acute coronary syndrome. The American Heart Association recommends a 12-hour observation period for these patients.
This study primarily aimed to ascertain whether the European Society of Cardiology non-ST-elevation myocardial infarction guidelines can be safely applied to rule-out acute coronary syndrome in low-risk patients with cocaine-associated chest pain.
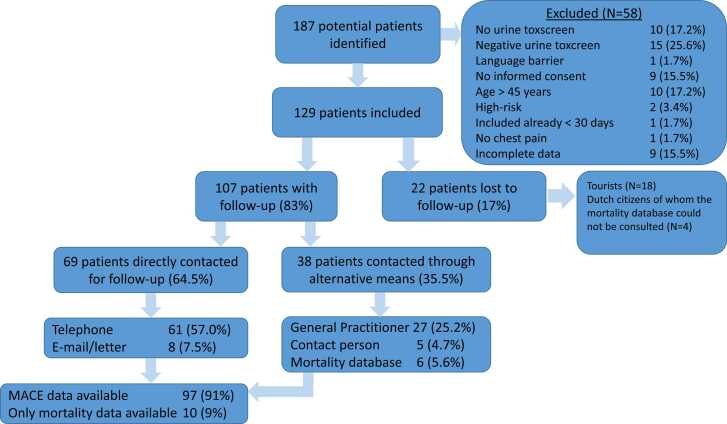
For this prospective observational cohort study, patients, aged 18-45 years old, who presented with cocaine-associated chest pain and were risk stratified as low risk according to the European Society of Cardiology non-ST-elevation myocardial infarction guidelines and therefore discharged home without prolonged observation period, were included. They were followed to assess major adverse cardiac events four weeks after presentation to the emergency department or chest pain unit. Cocaine use was confirmed with urine toxicology screening.
A total of 107 patients were included and analysed. The accuracy of the self-reported history of recent cocaine use was 94 %. Post-discharge cocaine use persisted among 32 % of patients. None of the included 107 patients died and major adverse cardiac event within four weeks did not occur among 97 patients with available data regarding MACE.
Ruling out an acute coronary syndrome using the European Society of Cardiology non-ST-elevation myocardial infarction guidelines is likely to be safe for patients with cocaine-associated chest pain, however this study was underpowered to reach definitive conclusions.
在所有与娱乐性药物相关的急诊科就诊病例中,4.7%的患者选择使用可卡因。在这些患者中,40%出现与可卡因相关的胸痛,其中4.7%发展为急性冠状动脉综合征。美国心脏协会建议对这些患者进行12小时的观察期。
本研究主要旨在确定欧洲心脏病学会非ST段抬高型心肌梗死指南是否可安全应用于排除低风险可卡因相关胸痛患者的急性冠状动脉综合征。
在这项前瞻性观察队列研究中,纳入了年龄在18 - 45岁之间、出现可卡因相关胸痛且根据欧洲心脏病学会非ST段抬高型心肌梗死指南被风险分层为低风险、因此无需延长观察期即可出院回家的患者。在他们到急诊科或胸痛单元就诊四周后对其进行随访,以评估主要不良心脏事件。通过尿液毒理学筛查确认是否使用可卡因。
共纳入并分析了107例患者。自我报告近期使用可卡因病史的准确率为94%。32%的患者出院后仍持续使用可卡因。纳入的107例患者中无人死亡,在97例有主要不良心脏事件可用数据的患者中,四周内未发生主要不良心脏事件。
对于可卡因相关胸痛患者,使用欧洲心脏病学会非ST段抬高型心肌梗死指南排除急性冠状动脉综合征可能是安全的,然而本研究样本量不足,无法得出确定性结论。