Su Yunchao, Lucas Rudolf, Fulton David J R, Verin Alexander D
Department of Pharmacology & Toxicology, Medical College of Georgia, Augusta University, Augusta, GA 30912, USA.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Medical College of Georgia, Augusta University, Augusta, GA 30912, USA.
Chin Med J Pulm Crit Care Med. 2024 Jun;2(2):80-87. doi: 10.1016/j.pccm.2024.04.002. Epub 2024 Jun 12.
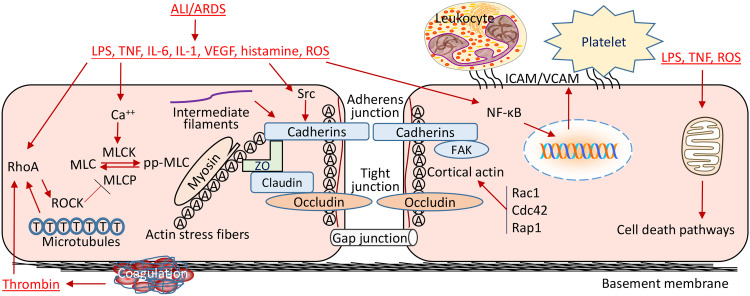
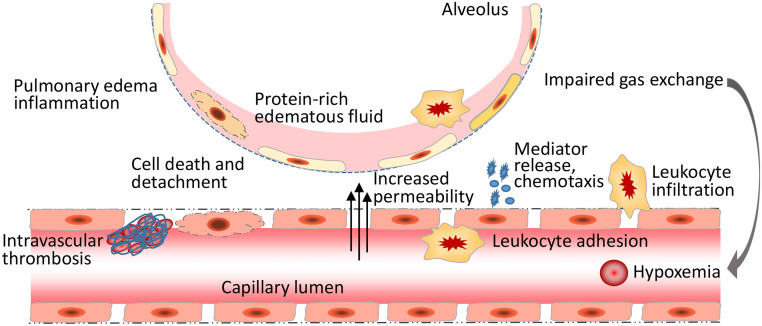
Endothelial cells (ECs) form a semi-permeable barrier between the interior space of blood vessels and the underlying tissues. Pulmonary endothelial barrier integrity is maintained through coordinated cellular processes involving receptors, signaling molecules, junctional complexes, and protein-regulated cytoskeletal reorganization. In acute lung injury (ALI) or its more severe form acute respiratory distress syndrome (ARDS), the loss of endothelial barrier integrity secondary to endothelial dysfunction caused by severe pulmonary inflammation and/or infection leads to pulmonary edema and hypoxemia. Pro-inflammatory agonists such as histamine, thrombin, bradykinin, interleukin 1, tumor necrosis factor , vascular endothelial growth factor, angiopoietin-2, and platelet-activating factor, as well as bacterial toxins and reactive oxygen species, cause dynamic changes in cytoskeletal structure, adherens junction disorganization, and detachment of vascular endothelial cadherin (VE-cadherin) from the actin cytoskeleton, leading to an increase in endothelial permeability. Endothelial interactions with leukocytes, platelets, and coagulation enhance the inflammatory response. Moreover, inflammatory infiltration and the associated generation of pro-inflammatory cytokines during infection cause EC death, resulting in further compromise of the structural integrity of lung endothelial barrier. Despite the use of potent antibiotics and aggressive intensive care support, the mortality of ALI is still high, because the mechanisms of pulmonary EC barrier disruption are not fully understood. In this review, we summarized recent advances in the studies of endothelial cytoskeletal reorganization, inter-endothelial junctions, endothelial inflammation, EC death, and endothelial repair in ALI and ARDS, intending to shed some light on the potential diagnostic and therapeutic targets in the clinical management of the disease.
内皮细胞(ECs)在血管内部空间与下层组织之间形成半透性屏障。肺内皮屏障的完整性通过涉及受体、信号分子、连接复合体以及蛋白质调节的细胞骨架重组的协同细胞过程得以维持。在急性肺损伤(ALI)或其更严重的形式急性呼吸窘迫综合征(ARDS)中,由于严重肺部炎症和/或感染导致的内皮功能障碍继发的内皮屏障完整性丧失会引发肺水肿和低氧血症。组胺、凝血酶、缓激肽、白细胞介素1、肿瘤坏死因子、血管内皮生长因子、血管生成素 - 2和血小板活化因子等促炎激动剂,以及细菌毒素和活性氧,会导致细胞骨架结构的动态变化、黏附连接紊乱以及血管内皮钙黏蛋白(VE - cadherin)从肌动蛋白细胞骨架上脱离,从而导致内皮通透性增加。内皮细胞与白细胞、血小板和凝血之间的相互作用会增强炎症反应。此外,感染期间的炎症浸润和促炎细胞因子的相关产生会导致内皮细胞死亡,进而进一步损害肺内皮屏障的结构完整性。尽管使用了强效抗生素和积极的重症监护支持,但ALI的死亡率仍然很高,因为肺内皮细胞屏障破坏的机制尚未完全明确。在这篇综述中,我们总结了ALI和ARDS中内皮细胞骨架重组、内皮细胞间连接、内皮炎症、内皮细胞死亡和内皮修复研究的最新进展,旨在为该疾病临床管理中的潜在诊断和治疗靶点提供一些启示。