Mori Tatsuya, Fujita Atsushi, Iwakura Masaki, Imura Jun, Onobuchi Kana, Kohta Masaaki, Kimura Hidehito, Sasayama Takashi
Department of Neurosurgery, Kobe University Graduate School of Medicine, Kobe, Japan.
Iwakura Neurosurgery and Headache Clinic, Kobe, Japan.
J Neurosurg Case Lessons. 2024 Jul 15;8(3). doi: 10.3171/CASE24202.
The reported actual risk of rupture for vertebral artery dissection (VAD) in patients presenting with headache is very low, ranging from 0.4% to 1.0%. The authors report a case in which the dissection site dilated rapidly within several hours after the dissection occurred resulting in subarachnoid hemorrhage (SAH).
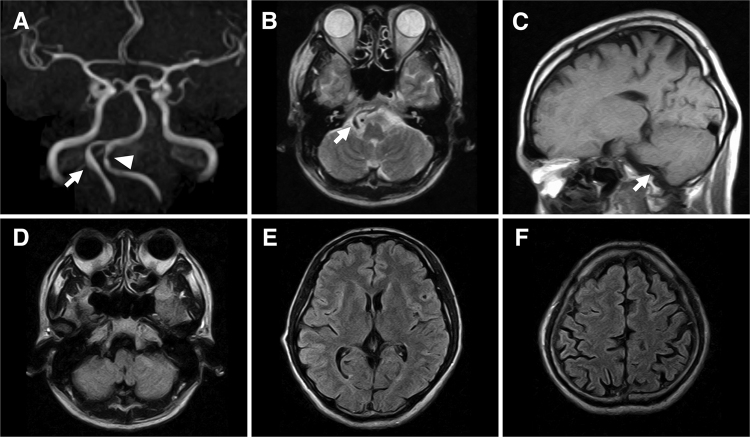
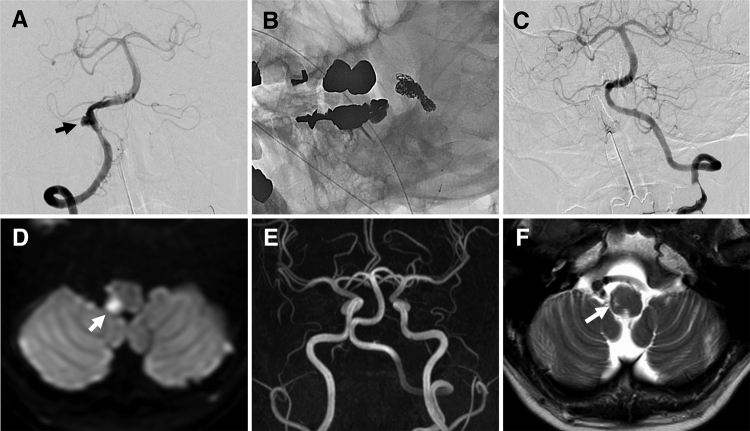
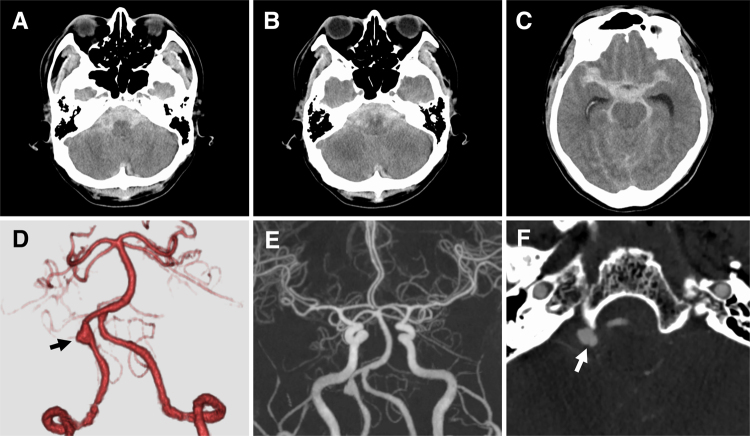
A 49-year-old healthy man who had participated in a marathon noticed a headache while running. Magnetic resonance imaging (MRI) performed 2 days later revealed no findings suspicious for right VAD, but a string sign was observed in the left side, suggesting left VAD. Three hours following MRI, he developed severe headaches and became unconscious at home, prompting emergency services to rush him to the hospital. A computed tomography scan showed diffuse SAH and a rapidly enlarged aneurysmal dilatation in the right vertebral artery. He underwent endovascular internal trapping to prevent rebleeding. He was discharged without any neurological symptoms. No recurrence or new dissection occurred after 2 years of follow-up.
Even in the absence of typical imaging findings, strict management, such as blood pressure control, is required when clinical findings strongly suggest VAD, and differentiation of VAD from primary headache is important. https://thejns.org/doi/10.3171/CASE24202.
报道显示,以头痛就诊的椎动脉夹层(VAD)患者实际的破裂风险非常低,范围在0.4%至1.0%之间。作者报告了1例患者,其夹层部位在夹层发生后的数小时内迅速扩张,导致蛛网膜下腔出血(SAH)。
一名49岁的健康男性在参加马拉松比赛时感到头痛。2天后进行的磁共振成像(MRI)检查未发现右椎动脉夹层可疑表现,但左侧观察到线样征,提示左椎动脉夹层。MRI检查3小时后,他在家中出现严重头痛并昏迷,促使急救人员将其紧急送往医院。计算机断层扫描显示弥漫性SAH,右椎动脉有迅速扩大的动脉瘤样扩张。他接受了血管内内置术以防止再次出血。他出院时无任何神经症状。随访2年未出现复发或新的夹层。
即使没有典型的影像学表现,当临床症状强烈提示椎动脉夹层时,也需要进行严格管理,如控制血压,并且区分椎动脉夹层与原发性头痛很重要。https://thejns.org/doi/10.3171/CASE24202。