Department of Pharmacy and Pharmacology, The Netherlands Cancer Institute, Antoni van Leeuwenhoek, Amsterdam, The Netherlands.
Department of Pharmacy, Radboud University Medical Centre, Nijmegen, The Netherlands.
Clin Pharmacokinet. 2024 Jul;63(7):1045-1054. doi: 10.1007/s40262-024-01399-8. Epub 2024 Jul 16.
Pazopanib is registered for metastatic renal cell carcinoma and soft-tissue sarcoma (STS). Its variable pharmacokinetic (PK) characteristics and narrow therapeutic range provide a strong rationale for therapeutic drug monitoring (TDM). Prior studies have defined target levels of drug exposure (≥ 20.5 mg/L) linked to prolonged progression-free survival (PFS), but the added value of using TDM remains unclear. This study investigates the effect of TDM of pazopanib in patients with STS on survival outcomes and dose-limiting toxicities (DLTs) and evaluates the feasibility of TDM-guided dosing.
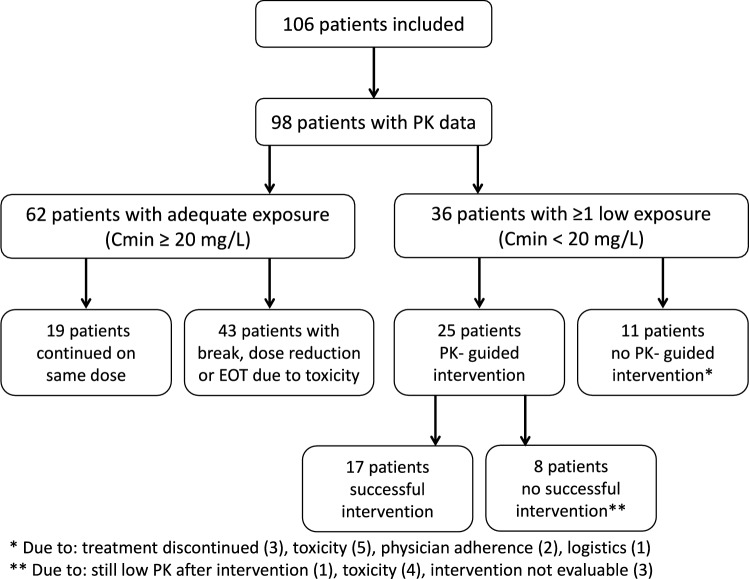
A TDM-guided cohort was compared to a non-TDM-guided cohort for PFS, overall survival (OS) and DLTs. PK samples were available from all patients, though not acted upon in the non-TDM-guided cohort. We evaluated the feasibility of TDM by comparing the proportion of underdosed patients in our TDM cohort with data from previous publications.
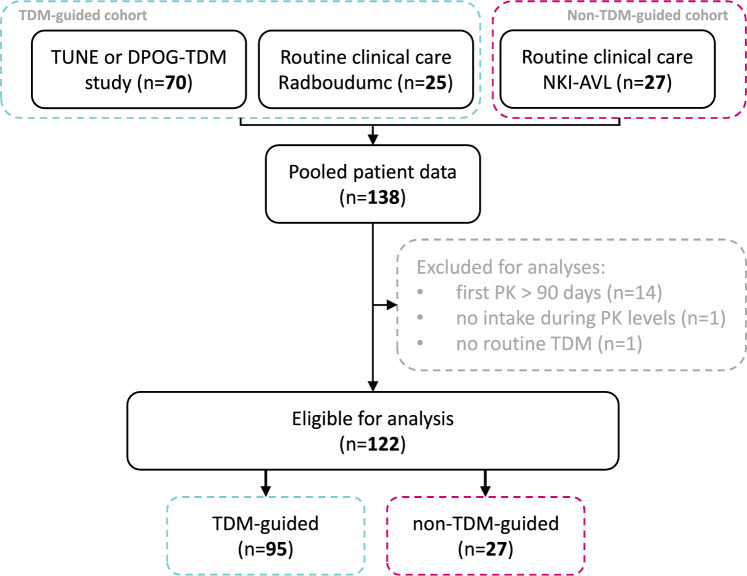
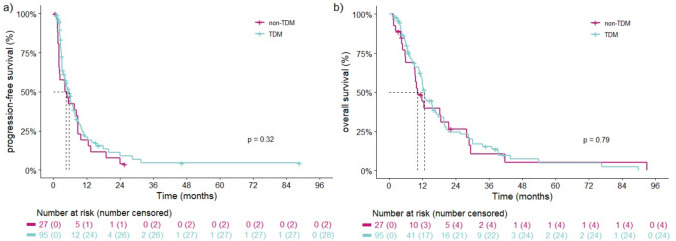
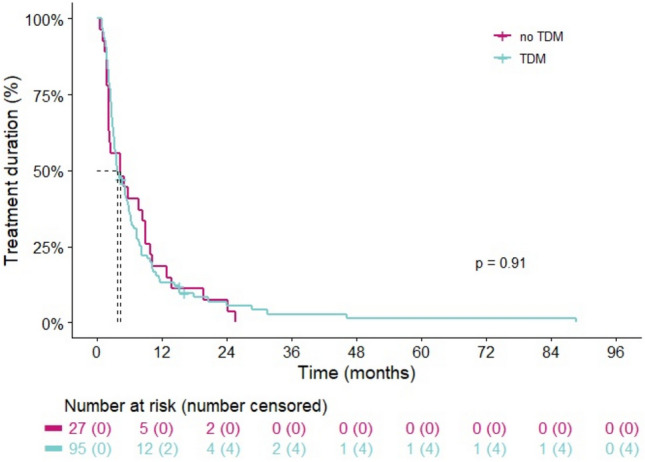
A total of 122 STS patients were included in the TDM-guided cohort (n = 95) and non-TDM-guided cohort (n = 27). The average exposure in the overall population was 30.5 mg/L and was similar in both groups. Median PFS and OS did not differ between the TDM-guided cohort and non-TDM-guided cohort (respectively 5.5 vs 4.4 months, p = 0.3, and 12.6 vs 10.1 months, p = 0.8). Slightly more patients in the non-TDM-guided cohort experienced DLTs (54%) compared to the TDM-guided cohort (44%). The proportion of underdosed patients (13.3%) was halved compared to historical data (26.7%).
TDM reduced the proportion of patients with subtherapeutic exposure levels by ~ 50%. Nonetheless, the added value of TDM for achieving target trough levels of ≥ 20.5 mg/L for pazopanib on survival outcomes could not be confirmed in STS patients.
帕唑帕尼已注册用于治疗转移性肾细胞癌和软组织肉瘤(STS)。其可变的药代动力学(PK)特征和狭窄的治疗范围为治疗药物监测(TDM)提供了强有力的依据。先前的研究已经确定了与无进展生存期(PFS)延长相关的药物暴露目标水平(≥20.5mg/L),但使用 TDM 的附加值仍不清楚。本研究调查了 STS 患者中帕唑帕尼 TDM 对生存结果和剂量限制毒性(DLTs)的影响,并评估了 TDM 指导剂量的可行性。
将 TDM 指导队列与非 TDM 指导队列进行比较,以评估 PFS、总生存期(OS)和 DLTs。所有患者均提供了 PK 样本,但在非 TDM 指导队列中并未进行处理。我们通过比较 TDM 队列中剂量不足患者的比例与以前出版物的数据来评估 TDM 的可行性。
共有 122 名 STS 患者被纳入 TDM 指导队列(n=95)和非 TDM 指导队列(n=27)。总体人群的平均暴露量为 30.5mg/L,两组之间相似。TDM 指导队列和非 TDM 指导队列的中位 PFS 和 OS 无差异(分别为 5.5 与 4.4 个月,p=0.3 和 12.6 与 10.1 个月,p=0.8)。非 TDM 指导队列中发生 DLT 的患者略多(54%)比 TDM 指导队列(44%)。剂量不足的患者比例(13.3%)与历史数据(26.7%)相比减半。
TDM 将治疗效果不佳的患者比例降低了约 50%。尽管如此,在 STS 患者中,TDM 并不能证实达到帕唑帕尼目标谷浓度≥20.5mg/L 以提高生存结果的附加值。