Baker Heart and Diabetes Institute, Melbourne, Victoria, Australia.
Department of Diabetes, Central Clinical School, Monash University, Clayton, Victoria, Australia.
Clin Sci (Lond). 2024 Aug 7;138(15):941-962. doi: 10.1042/CS20240178.
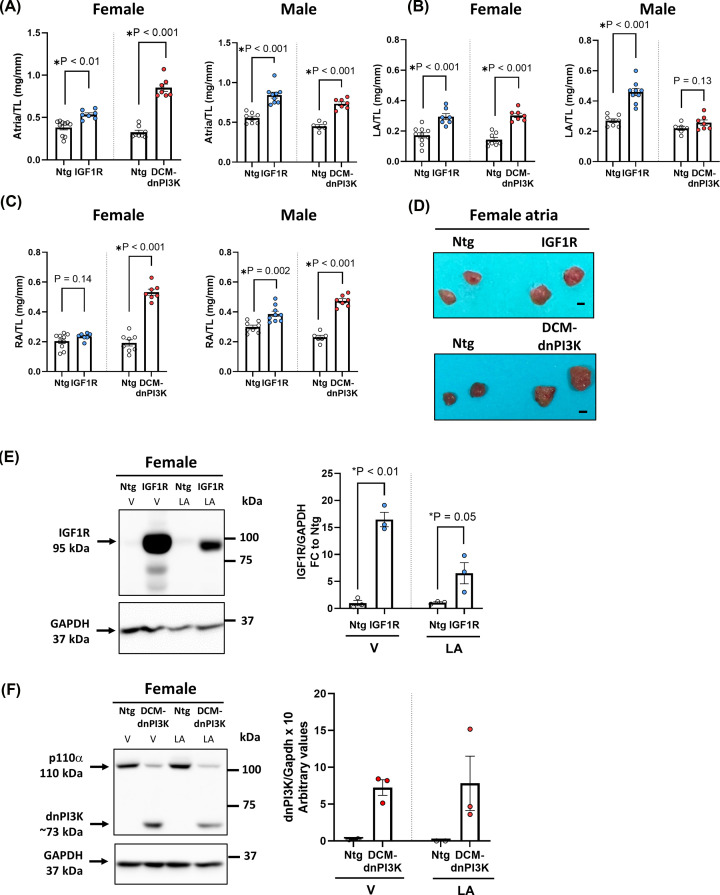
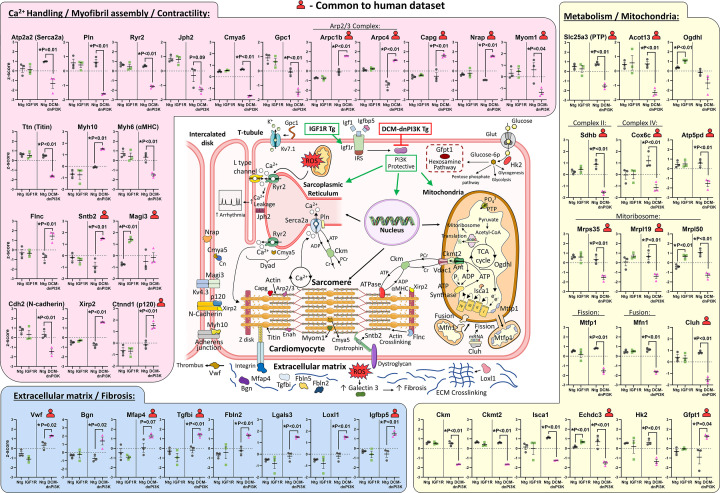
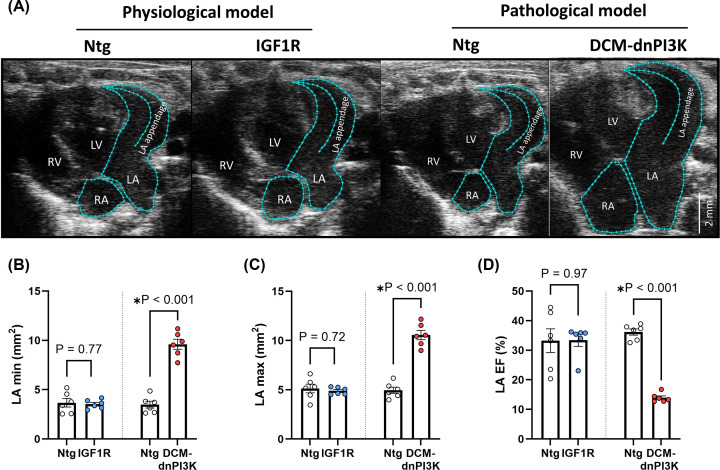
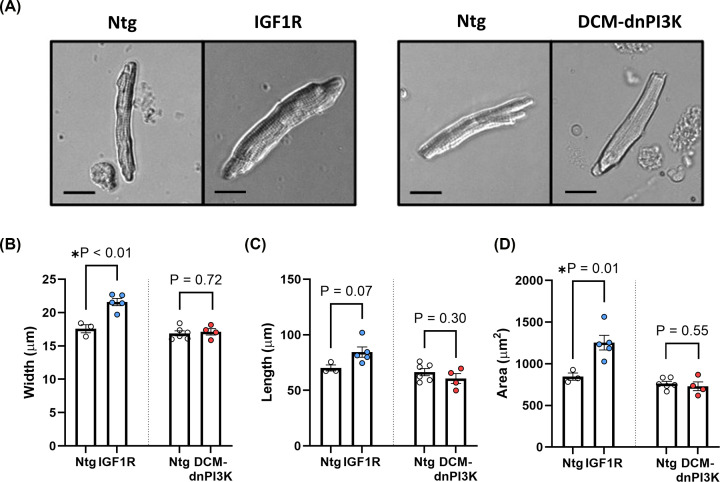
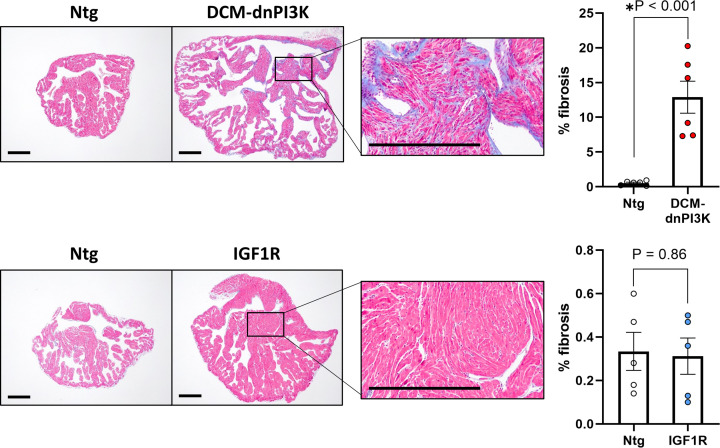
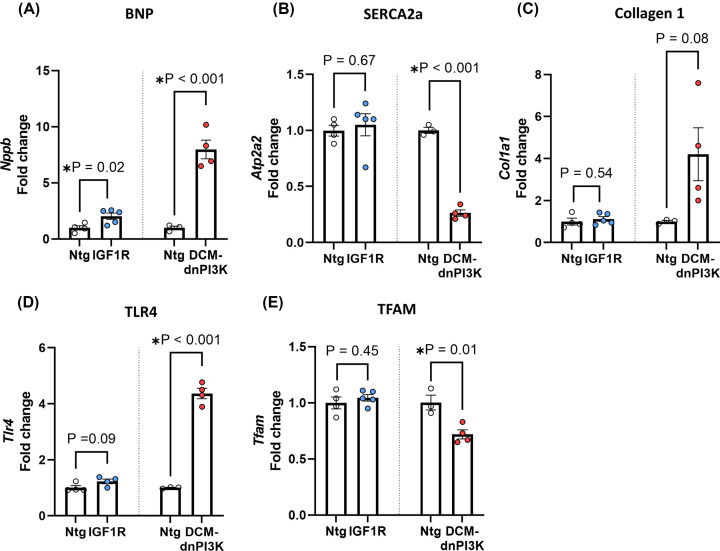
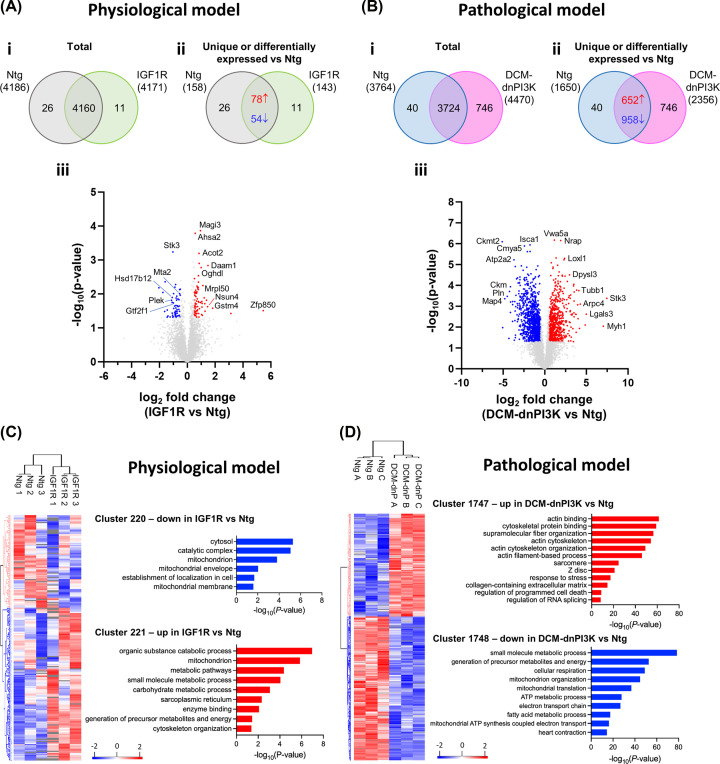
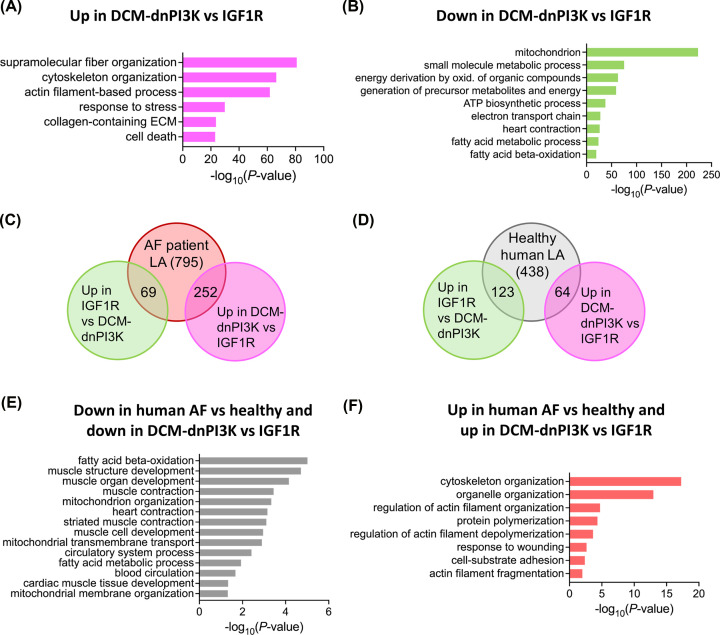
Atrial fibrillation (AF) remains challenging to prevent and treat. A key feature of AF is atrial enlargement. However, not all atrial enlargement progresses to AF. Atrial enlargement in response to physiological stimuli such as exercise is typically benign and reversible. Understanding the differences in atrial function and molecular profile underpinning pathological and physiological atrial remodelling will be critical for identifying new strategies for AF. The discovery of molecular mechanisms responsible for pathological and physiological ventricular hypertrophy has uncovered new drug targets for heart failure. Studies in the atria have been limited in comparison. Here, we characterised mouse atria from (1) a pathological model (cardiomyocyte-specific transgenic (Tg) that develops dilated cardiomyopathy [DCM] and AF due to reduced protective signalling [PI3K]; DCM-dnPI3K), and (2) a physiological model (cardiomyocyte-specific Tg with an enlarged heart due to increased insulin-like growth factor 1 receptor; IGF1R). Both models presented with an increase in atrial mass, but displayed distinct functional, cellular, histological and molecular phenotypes. Atrial enlargement in the DCM-dnPI3K Tg, but not IGF1R Tg, was associated with atrial dysfunction, fibrosis and a heart failure gene expression pattern. Atrial proteomics identified protein networks related to cardiac contractility, sarcomere assembly, metabolism, mitochondria, and extracellular matrix which were differentially regulated in the models; many co-identified in atrial proteomics data sets from human AF. In summary, physiological and pathological atrial enlargement are associated with distinct features, and the proteomic dataset provides a resource to study potential new regulators of atrial biology and function, drug targets and biomarkers for AF.
心房颤动 (AF) 的预防和治疗仍然具有挑战性。AF 的一个关键特征是心房扩大。然而,并非所有的心房扩大都会发展成 AF。对运动等生理刺激的心房扩大通常是良性且可逆的。了解导致病理性和生理性心房重构的心房功能和分子特征的差异,对于确定 AF 的新策略至关重要。对病理性和生理性心室肥厚的分子机制的研究已经为心力衰竭的新药物靶点提供了线索。相比之下,心房的研究受到了限制。在这里,我们从 (1) 一种病理性模型(心肌细胞特异性转基因 (Tg),由于保护性信号减少 [PI3K],发展为扩张型心肌病 [DCM] 和 AF;DCM-dnPI3K) 和 (2) 一种生理性模型(心肌细胞特异性 Tg,由于胰岛素样生长因子 1 受体增加而心脏增大;IGF1R)中对小鼠心房进行了特征描述。这两种模型的心房质量都增加了,但表现出不同的功能、细胞、组织学和分子表型。DCM-dnPI3K Tg 而非 IGF1R Tg 的心房扩大与心房功能障碍、纤维化和心力衰竭基因表达模式有关。心房蛋白质组学鉴定了与心肌收缩力、肌节组装、代谢、线粒体和细胞外基质相关的蛋白质网络,这些网络在模型中受到不同的调节;许多在人类 AF 的心房蛋白质组数据集中共鉴定出。总之,生理性和病理性心房扩大与不同的特征有关,蛋白质组数据集为研究心房生物学和功能的潜在新调节剂、药物靶点和 AF 生物标志物提供了资源。