Renaudineau Yves, Chauveau Dominique, Faguer Stanislas, Huart Antoine, Ribes David, Pugnet Gregory, Sailler Laurent, Jamme Thibaut, Treiner Emmanuel, Fortenfant Françoise, Bost Chloé, Carlé Caroline, Belliere Julie
Immunology Department Laboratory, Referral Medical Biology Laboratory, Institut Fédératif de Biologie, Toulouse University Hospital Center, France.
INFINITy, Toulouse Institute for Infectious and Inflammatory Diseases, INSERM U1291, CNRS U5051, University Toulouse III, Toulouse, France.
J Transl Autoimmun. 2024 Jun 20;9:100244. doi: 10.1016/j.jtauto.2024.100244. eCollection 2024 Dec.
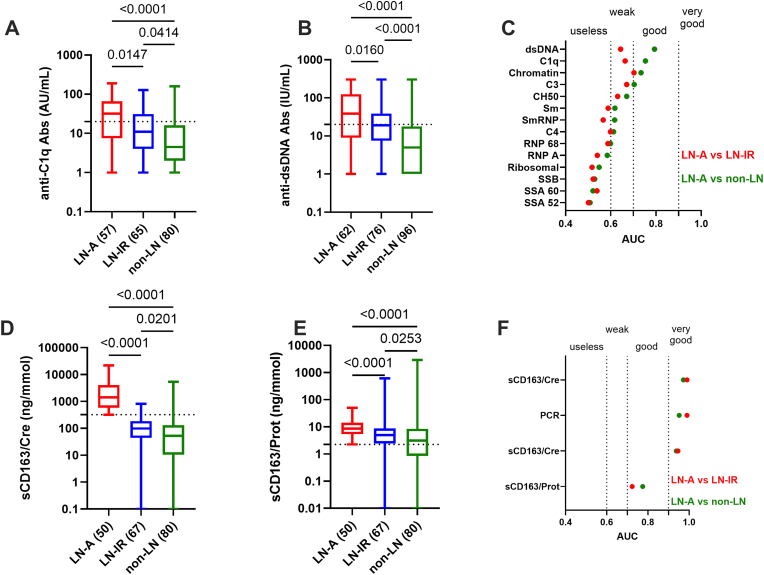
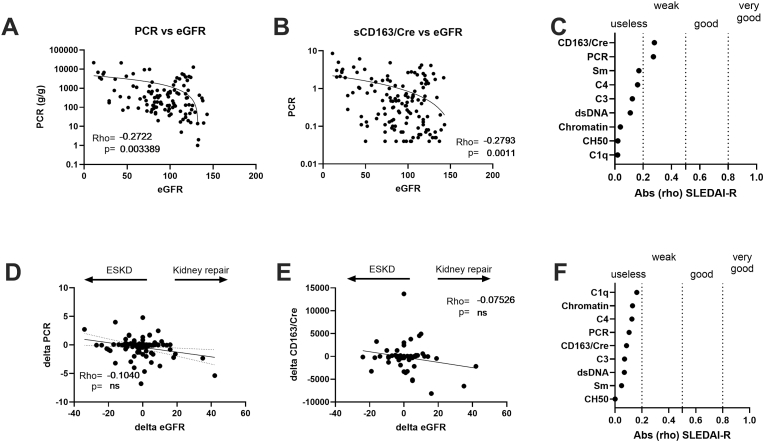
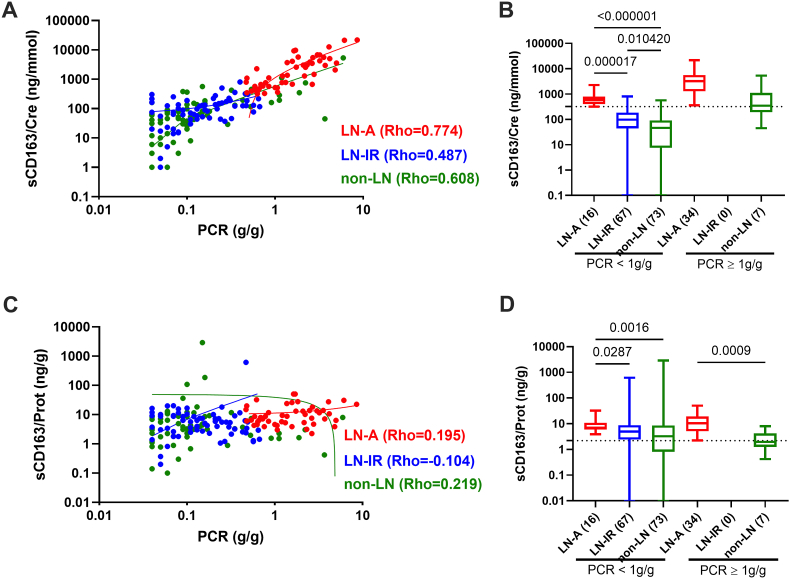
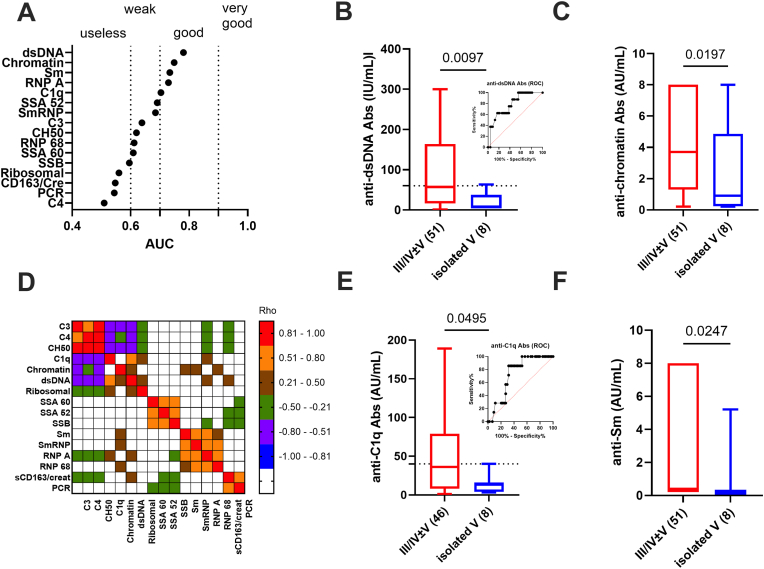
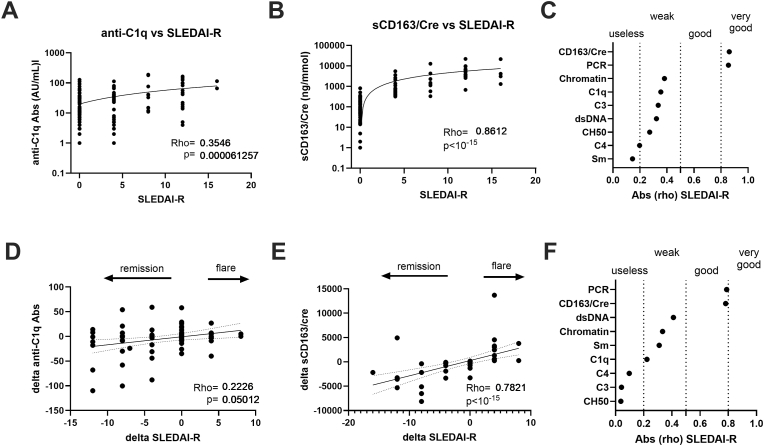
Lupus nephritis (LN) diagnosis and follow-up requires noninvasive biomarkers. Therefore, the added value of coupling the urinary soluble (s)CD163/creatinuria ratio with serological markers was evaluated in a real-world clinical practice. To this end, a monocentric and retrospective study was conducted in 139 SLE patients with biopsy-proven nephritis having an active LN (LN-A, n = 63 with a positive SLEDAI-renal score) or inactive (n = 76), as well as 98 non-renal SLE patients. The urinary sCD163/creatinuria ratio outperformed serological markers for predicting LN-A (AUC>0.972; p < 10 with a 100 % specificity threshold fixed at 320 ng/mmol), and for monitoring renal activity allowing prediction of impending flares and remissions in follow-up (AUC = 0.789, p < 10). LN-A patients with an elevated spot proteinuria/creatinuria ratio (p = 8 × 10) and sCD163/creatinuria ratio (p = 10) were at risk for developing end-stage kidney disease but sCD163/creatinuria ratio cannot substitute kidney biopsy to discriminate LN-A from other glomerulonephritis. Among serological markers (n = 14), anti-dsDNA and anti-C1q antibodies (Abs) (AUC>0.750 versus non-LN patients, and AUC>0.640 versus LN-IR patients) best predicted LN-A, and higher levels were retrieved in class III/IV proliferative LN-A. In multivariate logistic regression analysis, the urinary sCD163/creatinuria ratio remained the only statistically significant biomarker to predict LN-A (p < 0.001). In conclusion, and as compared to classical serological markers, the urinary sCD163/creatinuria ratio provides an additional parameter for monitoring LN patients.
狼疮性肾炎(LN)的诊断和随访需要非侵入性生物标志物。因此,在实际临床实践中评估了尿可溶性(s)CD163/肌酐尿比值与血清学标志物联合使用的附加价值。为此,对139例经活检证实患有活动性LN(LN-A,n = 63,SLEDAI-肾脏评分为阳性)或非活动性(n = 76)的狼疮性肾炎患者以及98例非肾脏狼疮患者进行了一项单中心回顾性研究。尿sCD163/肌酐尿比值在预测LN-A方面优于血清学标志物(AUC>0.972;在设定为320 ng/mmol的100%特异性阈值下p < 10),并且在监测肾脏活动方面能够预测随访中即将发生的病情复发和缓解(AUC = 0.789,p < 10)。尿蛋白/肌酐比值(p = 8×10)和sCD163/肌酐尿比值升高(p = 10)的LN-A患者有发展为终末期肾病的风险,但sCD163/肌酐尿比值不能替代肾活检来区分LN-A与其他肾小球肾炎。在血清学标志物(n = 14)中,抗双链DNA和抗C1q抗体(Abs)(与非LN患者相比AUC>0.750,与LN-IR患者相比AUC>0.640)对LN-A的预测效果最佳,并且在III/IV级增殖性LN-A中检测到更高水平。在多因素逻辑回归分析中,尿sCD163/肌酐尿比值仍然是预测LN-A的唯一具有统计学意义的生物标志物(p < 0.001)。总之,与经典血清学标志物相比,尿sCD163/肌酐尿比值为监测LN患者提供了一个额外的参数。