Health Services and Systems Research, Duke-NUS Medical School, Singapore.
Health Services and Systems Research, Duke-NUS Medical School, Singapore.
Lancet Glob Health. 2024 Aug;12(8):e1331-e1342. doi: 10.1016/S2214-109X(24)00188-8.
The Bridging Income Generation with Group Integrated Care (BIGPIC) trial in rural Kenya showed that integrating usual care with group medical visits or microfinance interventions reduced systolic blood pressure and cardiovascular risk in participants. We aimed to estimate the incremental cost-effectiveness of three BIGPIC interventions for a modelled cohort and by sex, as well as the cost of implementing these interventions.
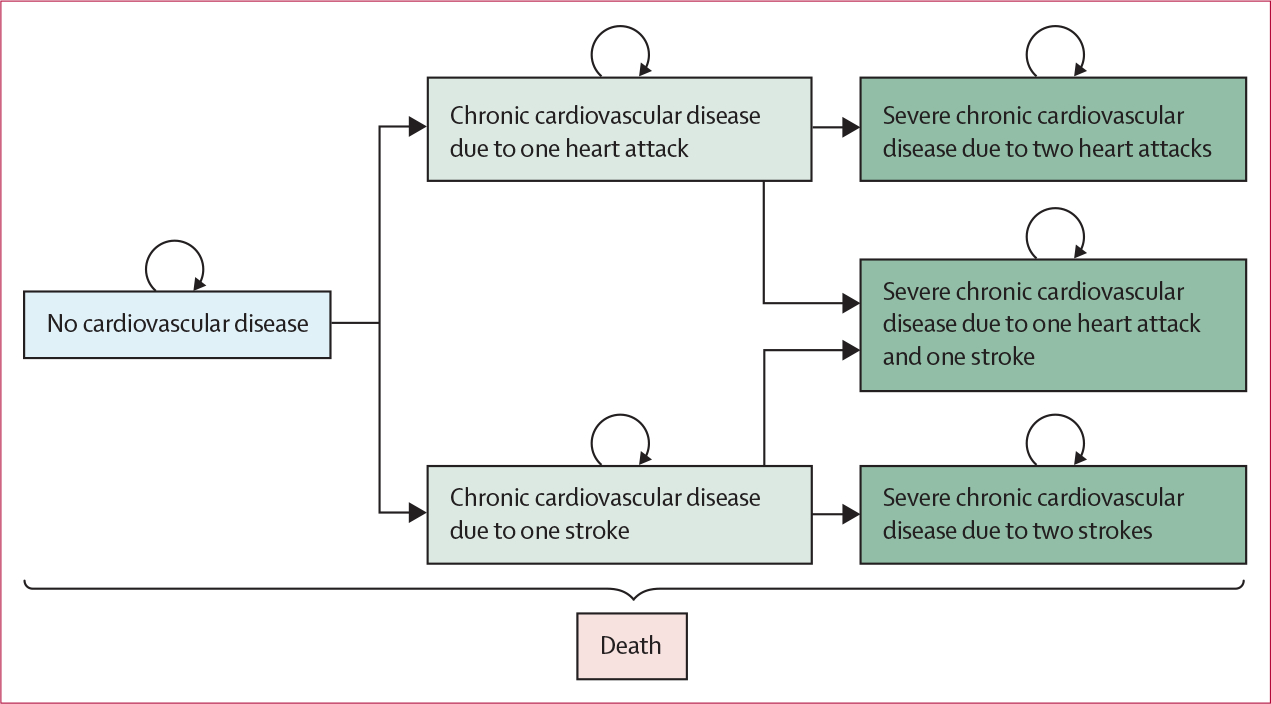
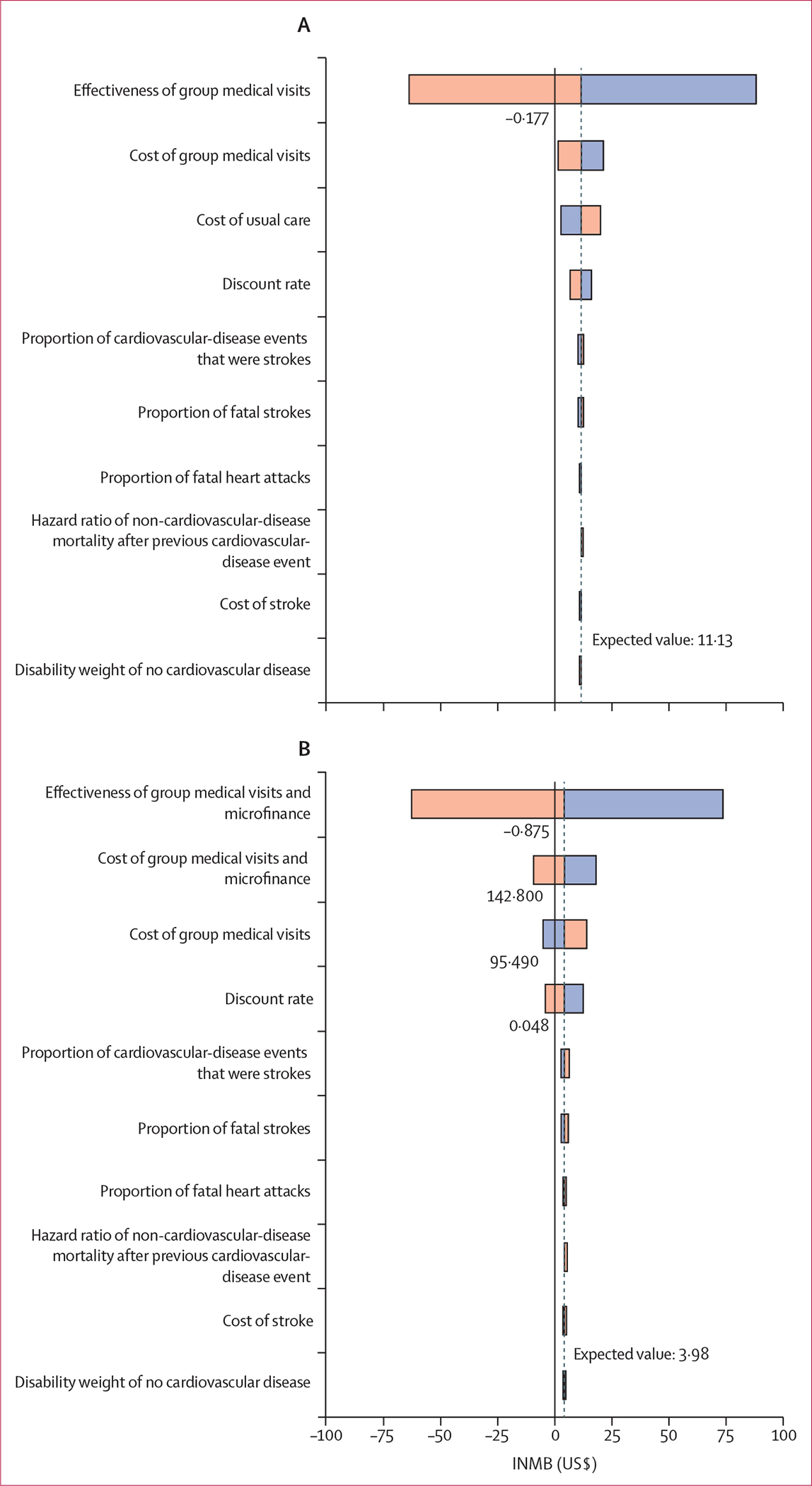
For this analysis, we used data collected during the BIGPIC trial, a four-group, cluster-randomised trial conducted in the western Kenyan catchment area of the Academic Model Providing Access to Healthcare. BIGPIC enrolled participants from 24 rural health facilities in rural western Kenya aged 35 years or older with either increased blood pressure or diabetes. Participants were assigned to receive either usual care, group medical visits, microfinance, or a combination of group medical visits and microfinance (GMV-MF). Our model estimated the incremental cost-effectiveness of the three BIGPIC interventions via seven health states (ie, a hypertensive state, five chronic cardiovascular-disease states, and a death state) by simulating transitions between health states for a hypothetical cohort of individuals with hypertension on the basis of QRISK3 scores. In every cycle, participants accrued costs and disability-adjusted life-years (DALYs) associated with their health state. Incremental cost-effectiveness ratios (ICERs) were calculated for the entire modelled cohort and by sex by dividing the incremental cost by the incremental effectiveness of the next most expensive intervention. The main outcome of this analysis was ICERs for each intervention evaluated. This analysis is registered at ClinicalTrials.gov (NCT02501746).
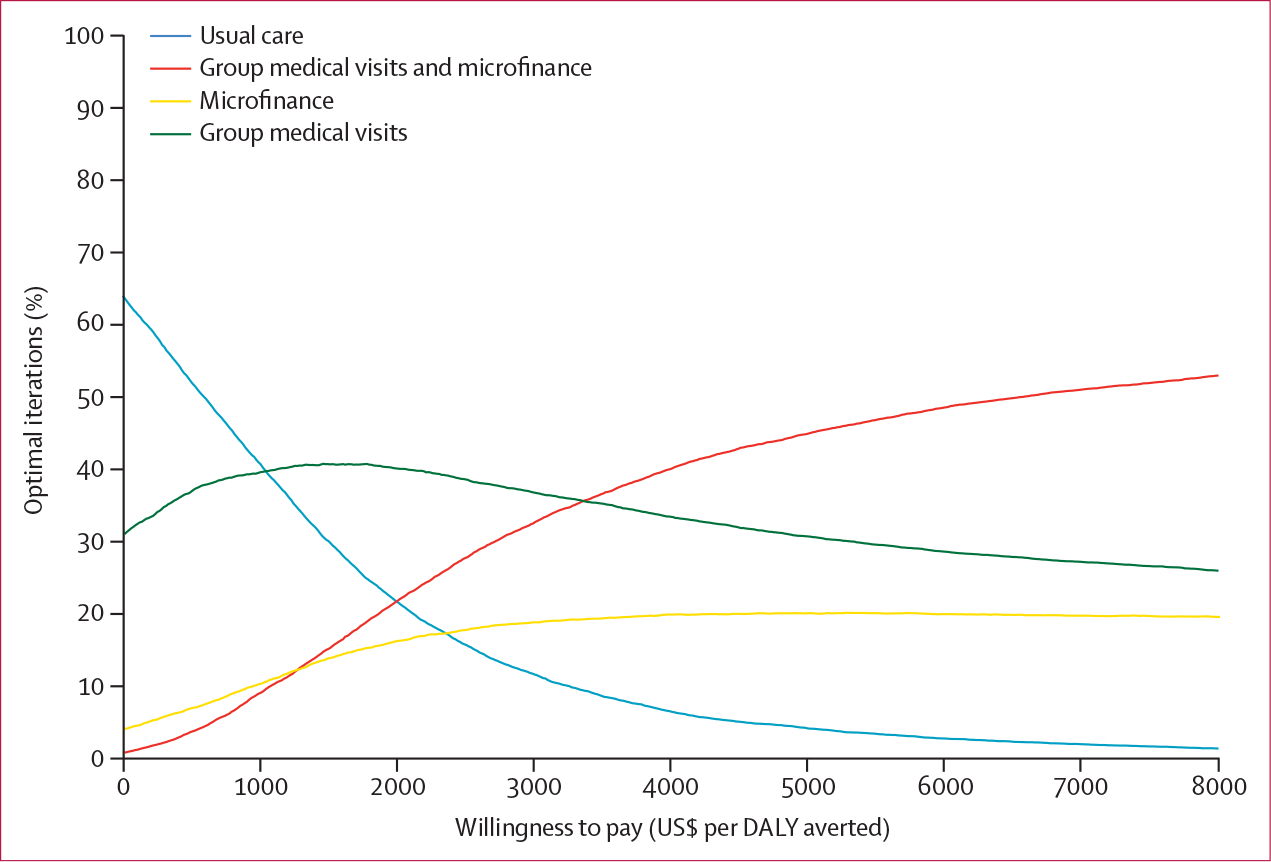
Between Feb 6, 2017, and Dec 29, 2019, 2890 people were recruited to the BIGPIC trial. 2020 (69·9%) of 2890 participants were female and 870 (30·1%) were male. At baseline, mean QRISK3 score was 11·5 (95% CI 11·1-11·9) for the trial population, 11·9 (11·5-12·2) for male participants, and 11·3 (11·0-11·6) for female participants. For the population of Kenya, group medical visits were estimated to cost US$7 more per individual than usual care and result in 0·005 more DALYs averted (ICER $1455 per DALY averted). Microfinance was estimated to cost $19 more than group medical visits but was only estimated to avert 0·001 more DALYs. Relative to group medical visits, GMV-MF was estimated to cost $29 more and avert 0·009 more DALYs ($3235 per DALY averted). Relative to usual care, GMV-MF was estimated to cost $37 more and avert 0·014 more DALYs ($2601 per DALY averted). In the first year of the intervention, usual care was estimated to be the least expensive intervention to implement ($87 per participant; $10 238 per health-facility catchment area [HFCA]), then group medical visits ($99 per participant; $12 268 per HFCA), then microfinance ($120 per participant; $14 172 per HFCA), with GMV-MF estimated to be the most expensive intervention to implement ($139 per participant; $16 913 per HFCA).
Group medical visits and GMV-MF were estimated to be cost-effective strategies to improve blood-pressure control in rural Kenya. However, which intervention to pursue depends on resource availability. Policy makers should consider these factors, in addition to sex differences in programme effectiveness, when selecting optimal implementation strategies.
US National Institutes of Health.
肯尼亚农村的 Bridging Income Generation with Group Integrated Care(BIGPIC)试验表明,将常规护理与团体医疗访视或小额金融干预相结合,可降低参与者的收缩压和心血管风险。我们旨在估计三种 BIGPIC 干预措施对模型队列的增量成本效益,并按性别进行估计,同时还估计实施这些干预措施的成本。
在这项分析中,我们使用了 BIGPIC 试验期间收集的数据,该试验是一项四组、集群随机试验,在肯尼亚西部学术模型提供医疗保健的集水区进行。BIGPIC 招募了年龄在 35 岁及以上的 24 个农村卫生机构的参与者,他们要么血压升高,要么患有糖尿病。参与者被分配接受常规护理、团体医疗访视、小额金融或团体医疗访视和小额金融的组合(GMV-MF)。我们的模型通过模拟基于 QRISK3 评分的高血压患者假设队列在健康状态之间的转变,估计了三种 BIGPIC 干预措施的增量成本效益,通过七个健康状态(即高血压状态、五种慢性心血管疾病状态和死亡状态)进行估计。在每个周期中,参与者都会产生与他们的健康状态相关的成本和残疾调整生命年(DALY)。增量成本效益比(ICER)是通过将下一个最昂贵的干预措施的增量成本除以增量效益来计算的。该分析的主要结果是对评估的每项干预措施的 ICER。这项分析在 ClinicalTrials.gov(NCT02501746)注册。
2017 年 2 月 6 日至 2019 年 12 月 29 日,2890 人被招募到 BIGPIC 试验中。2020 年(69.9%)的 2890 名参与者为女性,870 名(30.1%)为男性。在基线时,试验人群的 QRISK3 评分平均为 11.5(95%CI 11.1-11.9),男性参与者为 11.9(11.5-12.2),女性参与者为 11.3(11.0-11.6)。对于肯尼亚人口,团体医疗访视比常规护理多花费 7 美元,多避免 0.005 个 DALY(每避免一个 DALY 花费 1455 美元)。小额金融比团体医疗访视多花费 19 美元,但只多避免了 0.001 个 DALY。与团体医疗访视相比,GMV-MF 预计要多花费 29 美元,避免 0.009 个 DALY(每避免一个 DALY 花费 3235 美元)。与常规护理相比,GMV-MF 预计要多花费 37 美元,避免 0.014 个 DALY(每避免一个 DALY 花费 2601 美元)。在干预的第一年,常规护理预计是实施成本最低的干预措施(每位参与者 87 美元;每个卫生设施集水区[HFCA] 10238 美元),其次是团体医疗访视(每位参与者 99 美元;每个 HFCA 12268 美元),然后是小额金融(每位参与者 120 美元;每个 HFCA 14172 美元),GMV-MF 预计是实施成本最高的干预措施(每位参与者 139 美元;每个 HFCA 16913 美元)。
团体医疗访视和 GMV-MF 被估计为改善肯尼亚农村地区血压控制的具有成本效益的策略。然而,选择哪种干预措施取决于资源的可用性。政策制定者在选择最佳实施策略时,应考虑这些因素,以及方案有效性的性别差异。
美国国立卫生研究院。