Nakajima Kenichi, Nakata Tomoaki, Doi Takahiro, Verschure Derk O, Frantellizzi Viviana, De Feo Maria Silvia, Tada Hayato, Verberne Hein J
Department of Nuclear Medicine/Functional imaging and Artificial Intelligence, Kanazawa University, 13-1 Takara-machi, Kanazawa, 920-8640, Japan.
Department of Cardiology, Hakodate-Goryoukaku Hospital, Hakodate, Japan.
EJNMMI Res. 2024 Jul 21;14(1):67. doi: 10.1186/s13550-024-01131-4.
I-meta-iodobenzylguanidine (mIBG) has been applied to patients with chronic heart failure (CHF). However, the relationship between I-mIBG activity and lethal arrhythmic events (ArE) is not well defined. This study aimed to determine this relationship in Japanese and European cohorts.
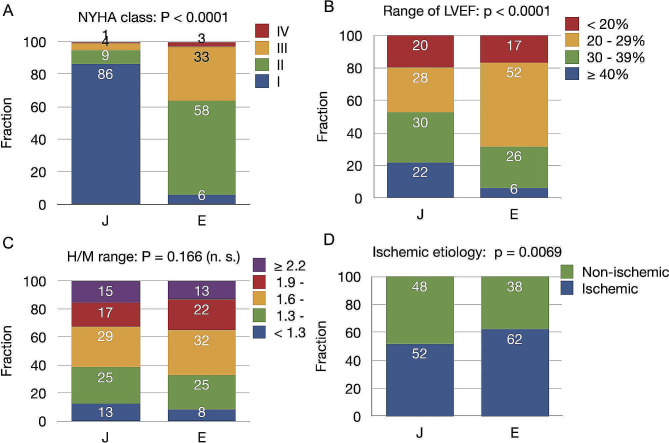
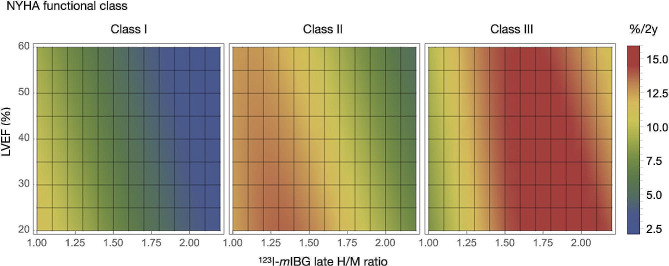
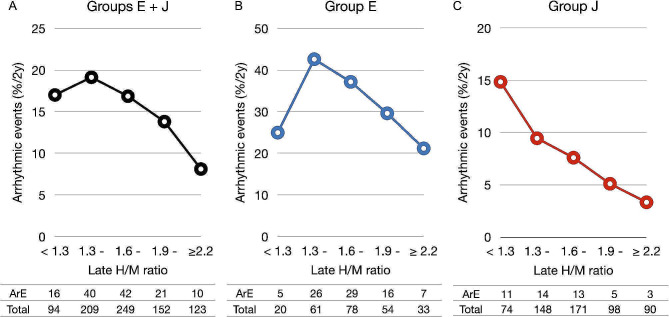
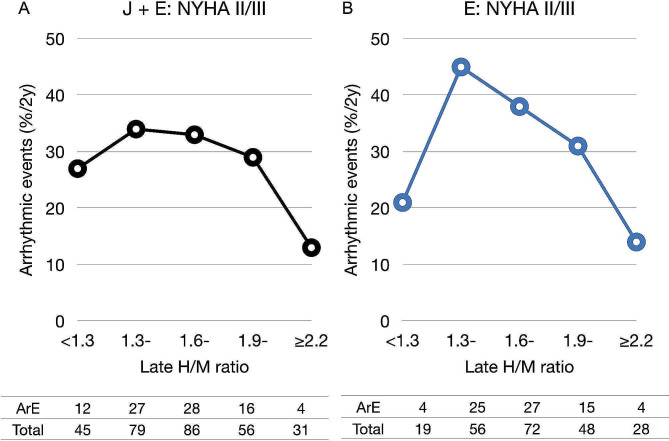
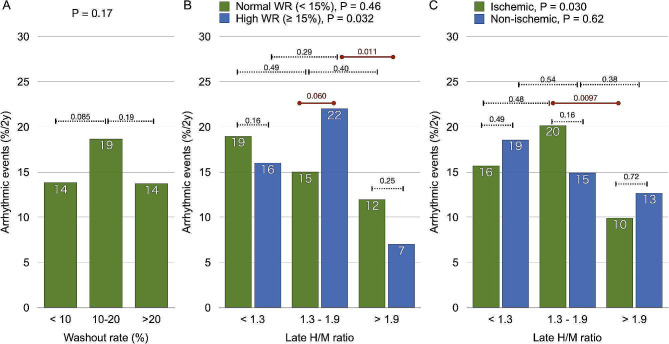
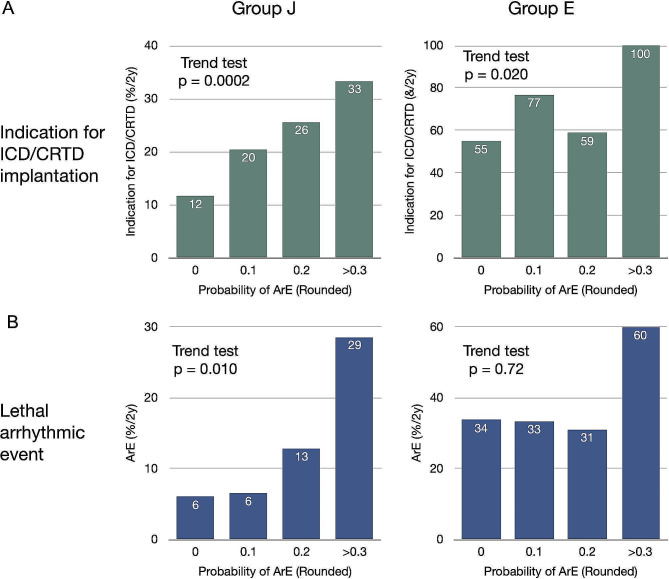
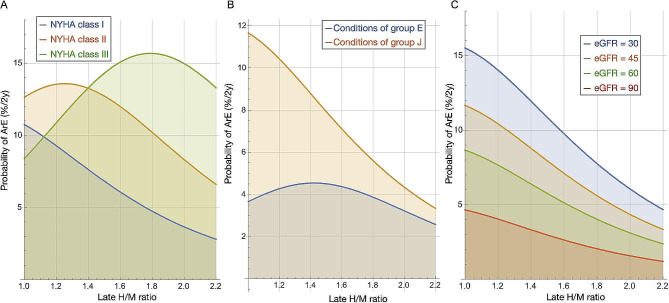
We calculated heart-to-mediastinum (H/M) count ratios and washout rates (WRs) of 827 patients using planar I-mIBG imaging. We defined ArEs as sudden cardiac death, arrhythmic death, and potentially lethal events such as sustained ventricular tachycardia, cardiac arrest with resuscitation, and appropriate implantable cardioverter defibrillator (ICD) discharge, either from a single ICD or as part of a cardiac resynchronization therapy device (CRTD). We analyzed the incidence of ArE with respect to H/M ratios, WRs and New York Heart Association (NYHA) functional classes among Japanese (J; n = 581) and European (E; n = 246) cohorts. We also simulated ArE rates versus H/M ratios under specific conditions using a machine-learning model incorporating 13 clinical variables. Consecutive patients with CHF were selected in group J, whereas group E comprised candidates for cardiac electronic devices. Groups J and E mostly comprised patients with NYHA functional classes I/II (95%) and II/III (91%), respectively, and 21% and 72% were respectively implanted with ICD/CRTD devices. The ArE rate increased with lower H/M ratios in group J, but the relationship was bell-shaped, with a high ArE rate within the intermediate H/M range, in group E. This bell-shaped curve was also evident in patients with NYHA classes II/III in the combined J and E groups, particularly in those with a high (> 15%) mIBG WR and with ischemic, but not in those with non-ischemic etiologies. Machine learning-based prediction of ArE risk aligned with these findings, indicating a bell-shaped curve in NYHA class II/III but not in class I.
The relationship between cardiac I-mIBG activity and lethal arrhythmic events is influenced by the background of patients. The bell-shaped relationship in NYHA classes II/III, high WR, and ischemic etiology likely aids in identifying patients at high risk for ArEs.
间碘苄胍(mIBG)已应用于慢性心力衰竭(CHF)患者。然而,I - mIBG活性与致死性心律失常事件(ArE)之间的关系尚未明确。本研究旨在确定日本和欧洲队列中的这种关系。
我们使用平面I - mIBG成像计算了827例患者的心/纵隔(H/M)计数比和洗脱率(WRs)。我们将ArE定义为心源性猝死、心律失常性死亡以及潜在的致死性事件,如持续性室性心动过速、复苏成功的心脏骤停以及合适的植入式心律转复除颤器(ICD)放电,无论是来自单一ICD还是作为心脏再同步治疗设备(CRTD)的一部分。我们分析了日本(J组;n = 581)和欧洲(E组;n = 246)队列中ArE的发生率与H/M比、WRs以及纽约心脏协会(NYHA)功能分级之间的关系。我们还使用包含13个临床变量的机器学习模型在特定条件下模拟了ArE发生率与H/M比的关系。J组选择的是连续的CHF患者,而E组包括心脏电子设备的候选者。J组和E组大多分别为NYHA功能分级为I/II级(95%)和II/III级(91%)的患者,分别有21%和72%植入了ICD/CRTD设备。J组中ArE发生率随H/M比降低而增加,但在E组中这种关系呈钟形,在中等H/M范围内ArE发生率较高。在J组和E组合并的NYHA II/III级患者中,这种钟形曲线也很明显,特别是在那些mIBG WR高(>15%)且有缺血性病因的患者中,但在非缺血性病因的患者中不明显。基于机器学习的ArE风险预测与这些发现一致,表明NYHA II/III级患者呈钟形曲线,而I级患者则不然。
心脏I - mIBG活性与致死性心律失常事件之间的关系受患者背景影响。NYHA II/III级、高WR和缺血性病因中的钟形关系可能有助于识别ArE高风险患者。