Stone Michael A, Parikh Harin, Foster Lukas, Wright-Chisem Adam, Ewing Brett, Karimi Amir H, Langberg Joshua
Department of Orthopaedic Surgery, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
Case Western Reserve University School of Medicine, Cleveland, OH, USA.
JSES Int. 2024 Apr 12;8(4):751-755. doi: 10.1016/j.jseint.2024.03.014. eCollection 2024 Jul.
The role of biceps tenodesis (BT) during open reduction internal fixation (ORIF) of proximal humerus fractures (PHFs) remains unclear. A subset of patients undergoing ORIF have persistent pain with unclear etiology. The purpose of our study was to compare outcomes of ORIF of PHFs with and without concomitant BT. We hypothesize patients undergoing BT at the time of ORIF will have improved patient-reported outcome scores with fewer secondary procedures related to treatment of the biceps.
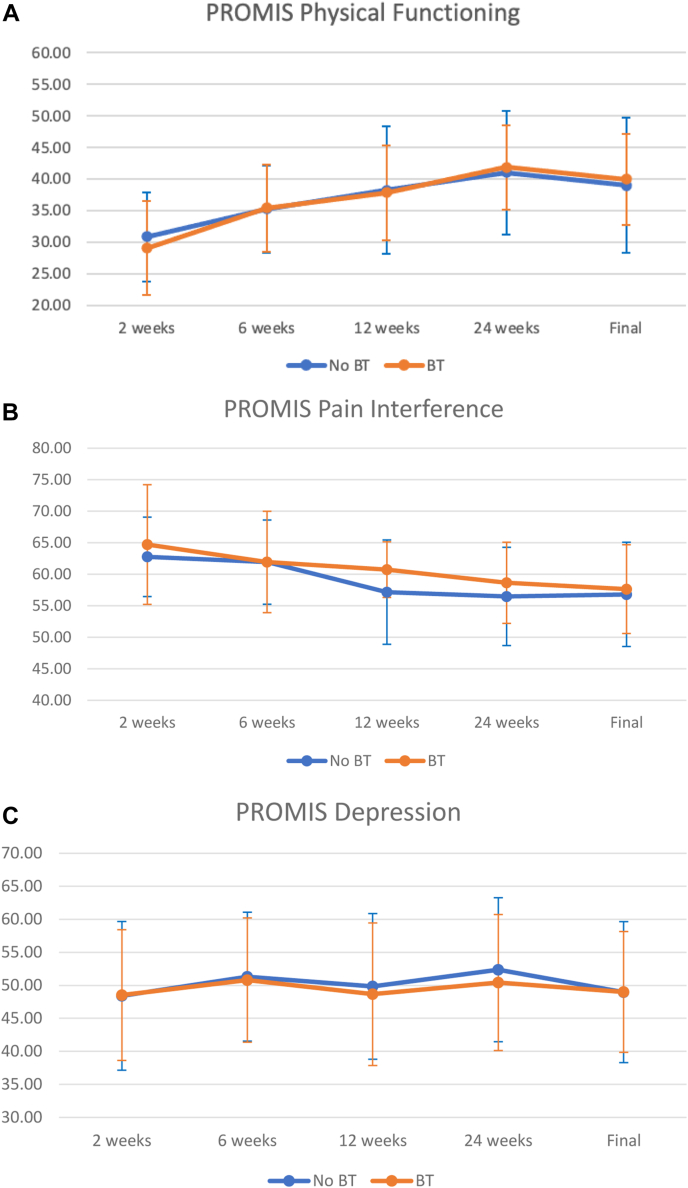
In this retrospective cohort study, all patients undergoing ORIF for a PHF at a single level one trauma center from January 2019 to June 2022 were reviewed. Patients under the age of 18 were excluded. Primary outcomes were patient-reported outcomes measurement information system physical function, depression, and pain interference scores at 5 time points up to final follow-up. Secondary outcomes included total operative time, complications, subsequent procedures, steroid injections, and range of motion. Chi-square tests were performed for categorical values and paired t-tests for continuous variables.
71 patients met inclusion criteria: 41 undergoing ORIF without BT and 30 undergoing ORIF with BT. Average follow-up was 11 months. There were no statistically significant differences in patient demographics between groups. There were no differences in patient-reported outcomes measurement information system scores at any time point postoperatively. At final follow-up patients in the ORIF with BT group had higher forward flexion than those who did not undergo BT (142 vs. 123 degrees, respectively, < .02). There were no differences in surgical time, revision rates, postsurgical complications, or postoperative injections between groups.
BT performed during ORIF of PHFs did not result in significantly different functional or patient-reported outcomes between groups, except for greater forward flexion at final follow-up. Although BT was done more commonly in severe PHFs, patients in both groups had similar rates of subsequent biceps-related procedures and revision surgery.
在肱骨近端骨折(PHF)切开复位内固定术(ORIF)中,肱二头肌固定术(BT)的作用仍不明确。一部分接受ORIF的患者存在病因不明的持续性疼痛。我们研究的目的是比较伴或不伴BT的PHF的ORIF治疗效果。我们假设在ORIF时接受BT的患者,其患者报告的结局评分会得到改善,且与肱二头肌治疗相关的二次手术会减少。
在这项回顾性队列研究中,对2019年1月至2022年6月在一家一级创伤中心接受PHF的ORIF治疗的所有患者进行了评估。排除18岁以下的患者。主要结局是患者报告的结局测量信息系统在直至最终随访的5个时间点的身体功能、抑郁和疼痛干扰评分。次要结局包括总手术时间、并发症、后续手术、类固醇注射和活动范围。对分类变量进行卡方检验,对连续变量进行配对t检验。
71例患者符合纳入标准:41例接受不伴BT的ORIF,30例接受伴BT的ORIF。平均随访时间为11个月。两组患者的人口统计学特征无统计学显著差异。术后任何时间点的患者报告结局测量信息系统评分均无差异。在最终随访时,接受伴BT的ORIF组患者的前屈角度高于未接受BT的患者(分别为142度和123度,P < 0.02)。两组之间的手术时间、翻修率、术后并发症或术后注射无差异。
在PHF的ORIF过程中进行BT,除了在最终随访时前屈角度更大外,两组之间的功能或患者报告结局没有显著差异。尽管BT在严重PHF中更常进行,但两组患者后续与肱二头肌相关的手术和翻修手术的发生率相似。