Trisalus Life Sciences, Westminster, Colorado, USA.
Department of Surgery, Brown University School of Medicine, Providence, RI, USA.
J Immunother Cancer. 2024 Jul 22;12(7):e008837. doi: 10.1136/jitc-2024-008837.
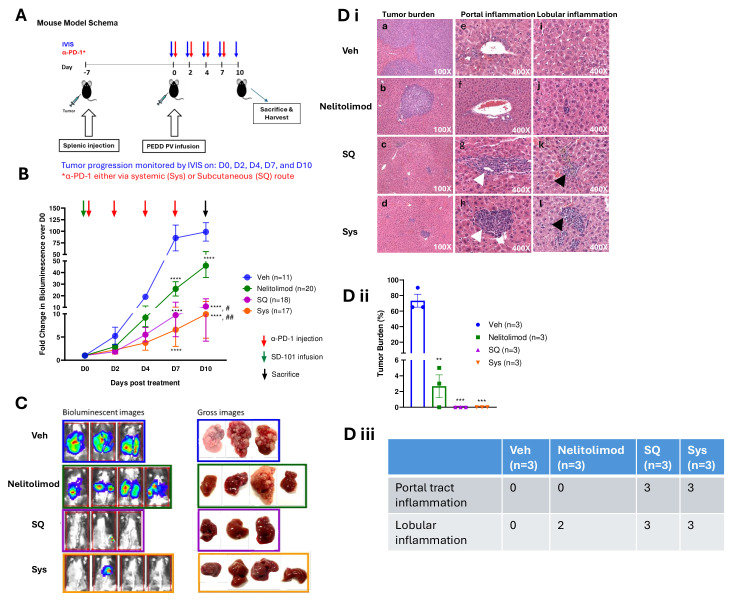
Toll-like receptor 9 (TLR9) agonists induce inflammatory responses that promote the killing of infectious micro-organisms, cancer cells and develop adaptive immune responses. Their ability as immunomodulators to enhance the activity of checkpoint inhibitors (CPI) in treating liver tumors is limited in part by the distinctive biology of intrahepatic myeloid-derived suppressor cells (MDSC) and challenges with tumor-specific therapeutic delivery. We have shown that the regional delivery of type C TLR9 agonist via pressure-enabled drug delivery (PEDD) system improves delivery to the tumor, enhances depletion of MDSCs and overall, stimulates the immune system in combination with or without CPI. Currently, CPIs are delivered intravenously, although there is a growing interest in its subcutaneous (SQ) administration. We compared nelitolimod formerly known as SD-101 administered using PEDD in combination with systemic (Sys) or SQ CPI in murine liver metastases (LM).
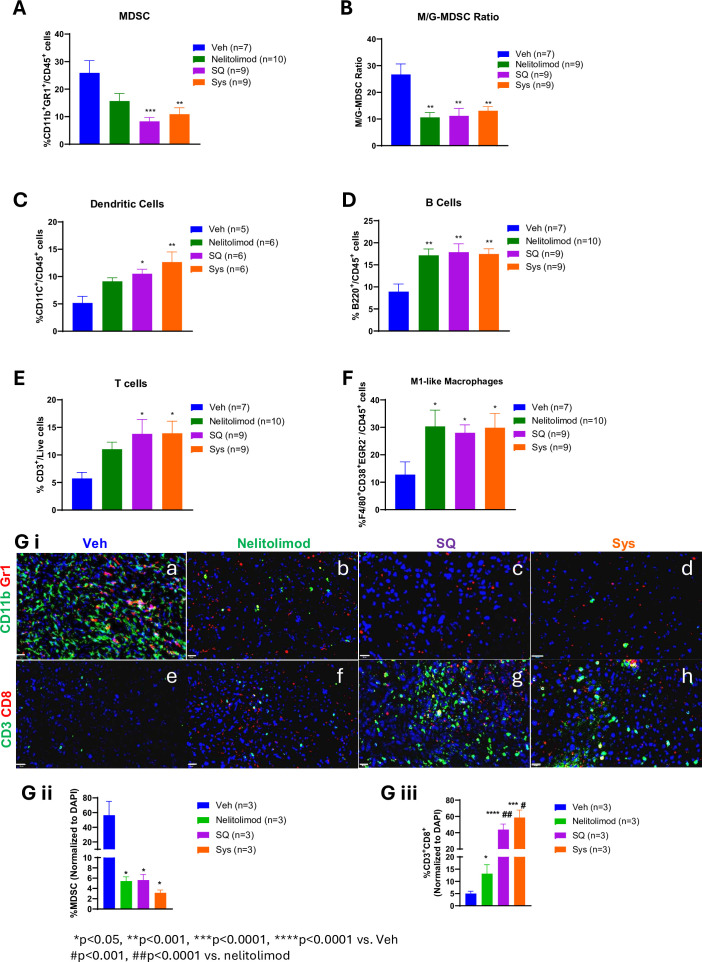
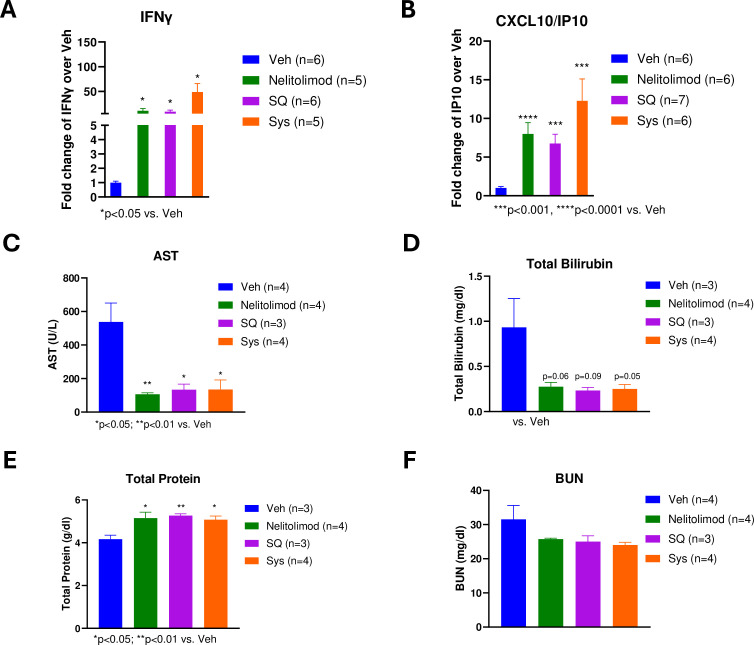
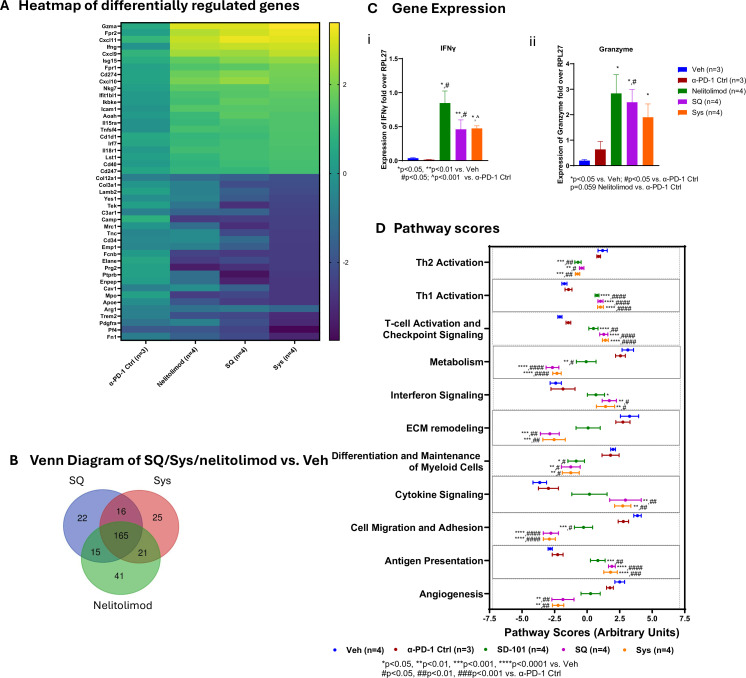
The LM model was developed by injecting MC38-Luc cells via the spleen of 8-12 week old male C57/BL6 mice followed by splenectomy. After a week, fluorescently labeled nelitolimod (10 µg/mouse) was delivered via PEDD and co-administered anti-programmed cell death-1 (α-PD-1) either via Sys or SQ. Tumor burden was monitored by in vivo imaging system. Serum cytokine levels were analyzed by Luminex. Tissues were harvested on Day 3 (D3) or Day 10 (D10) post-PEDD to enrich CD45 cells and were analyzed via NanoString targeted transcriptomics (D3) or flow cytometry (FC, D10) to interrogate immune cell populations (D10). For NanoString analysis, the innate immune panels were selected, and for FC, MDSCs (CD11bGr1), B cells (B220), dendritic cells (DC, CD11c), T (CD3) cells, and M1-like macrophages (F4/80CD38Egr2) were quantified.
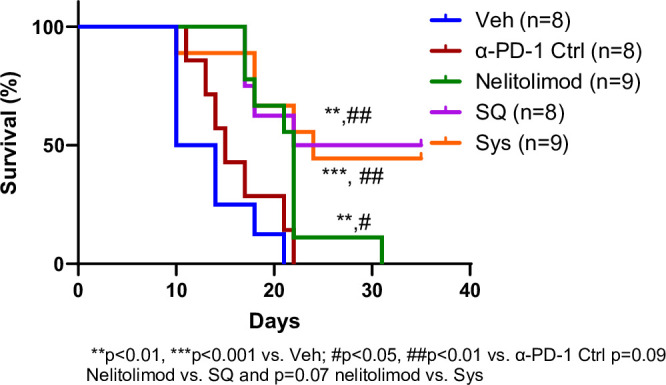
Nelitolimod delivered via PEDD resulted in changes in innate and adaptive immune cells within LM, including depletion of liver MDSC and increased M1-like macrophages in the liver, which are supportive of antitumor immunity. While CPI monotherapy failed to control tumor progression, nelitolimod and CPI combination improved LM control, survival and antitumor immunity beyond the nelitolimod monotherapy effect, irrespective of CPI delivery route.
The SQ route of CPI delivery was equivalent to Sys in combination with nelitolimod, suggesting SQ-CPI may be a rational choice in combination with PEDD of nelitolimod for liver tumor treatment.
Toll 样受体 9(TLR9)激动剂可诱导炎症反应,促进感染微生物、癌细胞的杀伤,并促进适应性免疫反应。其作为免疫调节剂的能力,部分受到肝髓系来源抑制细胞(MDSC)独特生物学特性的限制,以及肿瘤特异性治疗递送的挑战。我们已经表明,通过压力增强药物递送(PEDD)系统区域递送 C 型 TLR9 激动剂可改善肿瘤的递送,增强 MDSC 的耗竭,并且总体上增强免疫系统,无论是否存在检查点抑制剂(CPI)。目前,CPI 是通过静脉内给药,尽管皮下(SQ)给药越来越受到关注。我们比较了以前称为 SD-101 的 nelitolimod,它通过 PEDD 联合系统(Sys)或 SQ CPI 在小鼠肝转移(LM)中的给药效果。
LM 模型通过向 8-12 周龄雄性 C57/BL6 小鼠的脾脏注射 MC38-Luc 细胞建立,然后进行脾切除术。一周后,通过 PEDD 递送荧光标记的 nelitolimod(10μg/只小鼠),并联合通过 Sys 或 SQ 给予抗程序性细胞死亡蛋白-1(α-PD-1)。通过体内成像系统监测肿瘤负荷。通过 Luminex 分析血清细胞因子水平。在 PEDD 后第 3 天(D3)或第 10 天(D10)收获组织,富集 CD45 细胞,并通过 NanoString 靶向转录组学(D3)或流式细胞术(FC,D10)分析以研究免疫细胞群(D10)。对于 NanoString 分析,选择了先天免疫面板,对于 FC,分析了骨髓来源的抑制细胞(CD11bGr1)、B 细胞(B220)、树突状细胞(DC,CD11c)、T(CD3)细胞和 M1 样巨噬细胞(F4/80CD38Egr2)。
通过 PEDD 递送的 nelitolimod 导致 LM 内固有和适应性免疫细胞发生变化,包括肝 MDSC 的耗竭和肝内 M1 样巨噬细胞的增加,这有助于抗肿瘤免疫。虽然 CPI 单药治疗未能控制肿瘤进展,但 nelitolimod 与 CPI 联合治疗可改善 LM 控制、生存和抗肿瘤免疫,超过了 nelitolimod 单药治疗的效果,而与 CPI 给药途径无关。
CPI 的 SQ 给药途径与 Sys 联合 nelitolimod 等效,这表明 SQ-CPI 可能是与 PEDD 联合 nelitolimod 治疗肝肿瘤的合理选择。