Shinyurigaoka General Hospital, Asou-ku, Kawasaki, Kanagawa, Japan.
Department of Biochemistry, Tokyo Medical University, Shinjuku-ku, Tokyo, Japan.
PLoS One. 2024 Jul 25;19(7):e0307662. doi: 10.1371/journal.pone.0307662. eCollection 2024.
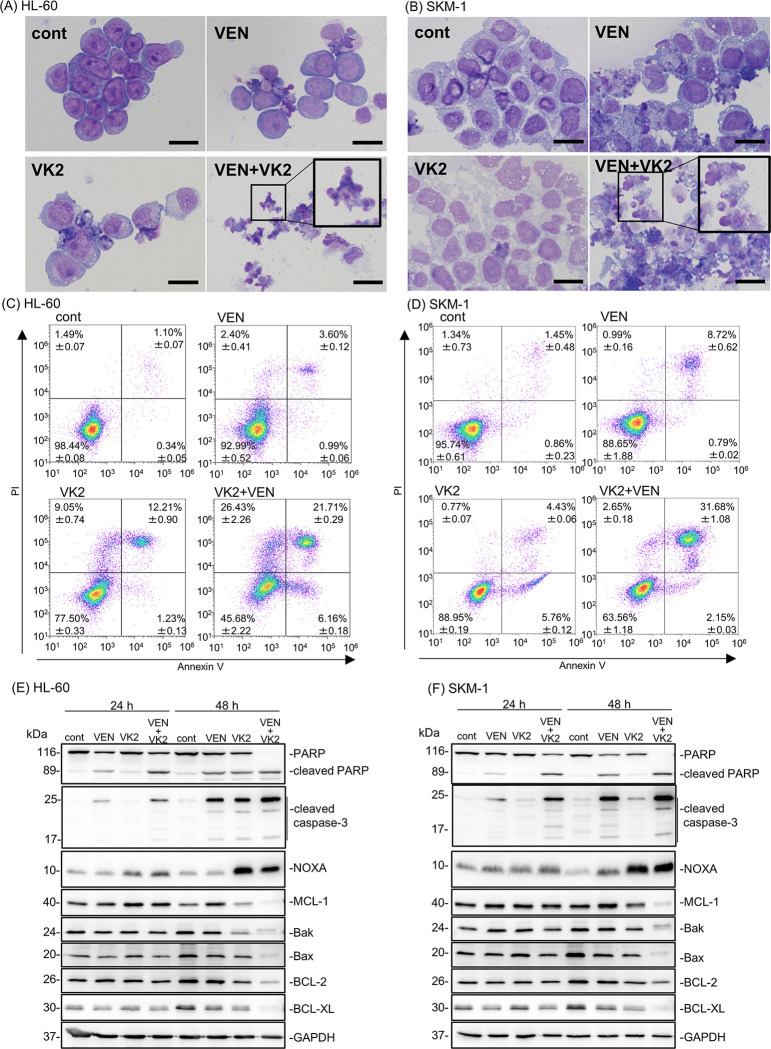
Promising outcomes have been reported in elder patients with acute myeloid leukemia (AML) using combined therapy of venetoclax (VEN) and azacytidine (AZA) in recent years. However, approximately one-third of patients appear to be refractory to this therapy. Vitamin K2 (VK2) shows apoptosis-inducing activity in AML cells, and daily oral VK2 (menaquinone-4, GlakayR) has been approved for patients with osteoporosis in Japan. We observed a high response rate to AZA plus VEN therapy, with no 8-week mortality in the newly diagnosed AML patients consuming daily VK2 in our hospital. The median age of the patients was 75.9 years (range 66-84) with high-risk features. Patients received AZA 75 mg/m2 on D1-7, VEN 400 mg on D1-28, and daily VK2 45 mg. The CR/CRi ratio was 94.7% (18/19), with a CR rate of 79%. Complete cytogenetic CR was achieved in 15 of 19 (79%) patients, and MRD negativity in 2 of 15 (13%) evaluable CR patients. Owing to the extremely high response rate in clinical settings, we further attempted to investigate the underlying mechanisms. The combination of VK2 and VEN synergistically induced apoptosis in all five AML cell lines tested. VK2, but not VEN, induced mitochondrial reactive oxygen species (ROS), leading to the transcriptional upregulation of NOXA, followed by MCL-1 repression. ROS scavengers repressed VK2 induced-NOXA expression and led to the cancellation of pronounced apoptosis and the downregulation of MCL-1 by VK2 plus VEN. Additionally, knockdown and knockout of NOXA resulted in abrogation of the MCL-1 repression as well as enhanced cytotoxicity by the two-drug combination, indicating that VK2 suppresses MCL-1 via ROS-mediated NOXA induction. These data suggest that the dual inhibition of BCL-2 by VEN and MCL-1 by VK2 is responsible for the remarkable clinical outcomes in our patients. Therefore, large-scale clinical trials are required.
近年来,维奈托克(VEN)联合阿扎胞苷(AZA)的联合疗法在老年急性髓系白血病(AML)患者中取得了有希望的结果。然而,约三分之一的患者似乎对此治疗无反应。维生素 K2(VK2)在 AML 细胞中具有诱导凋亡的活性,日本已批准每日口服 VK2(甲萘醌-4,GlakayR)用于骨质疏松症患者。我们观察到在我们医院接受每日 VK2 治疗的新诊断 AML 患者中,AZA 加 VEN 治疗的反应率很高,无 8 周死亡率。患者的中位年龄为 75.9 岁(范围 66-84),具有高危特征。患者接受 AZA 75mg/m2 于 D1-7 天,VEN 400mg 于 D1-28 天,每日 VK2 45mg。CR/CRi 比率为 94.7%(18/19),CR 率为 79%。19 例可评估患者中,15 例(79%)完全细胞遗传学 CR,15 例中有 2 例(13%)MRD 阴性。由于临床环境中极高的反应率,我们进一步试图研究潜在的机制。VK2 和 VEN 的联合作用可协同诱导所有五种 AML 细胞系发生凋亡。VK2,但不是 VEN,诱导线粒体活性氧物质(ROS),导致 NOXA 的转录上调,随后 MCL-1 抑制。ROS 清除剂抑制 VK2 诱导的 NOXA 表达,并导致 VK2 加 VEN 引起的明显凋亡和 MCL-1 下调的取消。此外,NOXA 的敲低和敲除导致 MCL-1 抑制的取消以及两种药物联合的增强细胞毒性,表明 VK2 通过 ROS 介导的 NOXA 诱导抑制 MCL-1。这些数据表明,VEN 对 BCL-2 的双重抑制和 VK2 对 MCL-1 的双重抑制是我们患者临床结果显著的原因。因此,需要进行大规模的临床试验。