Institute of Primary Health Care (BIHAM), University of Bern, 3012, Bern, Switzerland.
Graduate School for Health Sciences, University of Bern, 3012, Bern, Switzerland.
BMC Health Serv Res. 2024 Jul 26;24(1):849. doi: 10.1186/s12913-024-11339-8.
Collaboration between physicians and pharmacists facilitates the conduct of medication optimisation efforts. In the context of deprescribing, pharmacists' roles are often described as making deprescribing recommendations to physicians. Little is known about factors associated with pharmacists' willingness to make deprescribing recommendations and their interprofessional collaboration with physicians in Swiss primary care settings.
To explore pharmacists' perspectives on medication optimisation and deprescribing in older adults, and their preferences for interprofessional collaboration in Swiss primary care settings.
In this cross-sectional study, a random sample of 1000 pharmacist members of the Swiss Pharmacists Association pharmaSuisse was invited to participate in a survey on medication optimisation, deprescribing, and interprofessional collaboration. The survey contained three case vignettes of multimorbid patients with polypharmacy aged ≥ 80 years old, with different levels of dependency in activities in daily living (ADL) and cardiovascular disease (CVD). For each case vignette, pharmacists were asked if and which medications they would deprescribe. We calculated proportions of pharmacists' willingness to deprescribe by case vignette and performed a multilevel logistic regression to assess associations between CVD, ADL, and willingness to deprescribe.
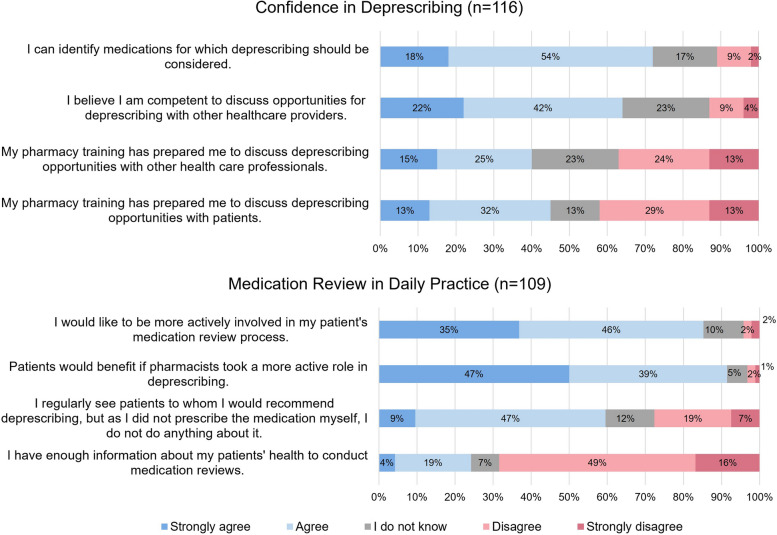
One hundred thirty-eight (14%) pharmacists responded to the survey: 113 (82%) were female, their mean age was 44 years (SD = 11), and 66% (n = 77) reported having never received any specific training on how to conduct structured medication reviews. Eighty-three (72%) pharmacists reported to be confident in identifying deprescribing opportunities. All pharmacists were willing to deprescribe ≥ 1 medication in all vignettes. Patients with CVD were at lower odds of having medications deprescribed (OR = 0.27, 95%CI 0.21 to 0.36). Willingness to deprescribe was lower with higher dependency in ADL (medium versus low dependency: OR = 0.68, 95%CI 0.54 to 0.87, high versus low dependency: OR = 0.72, 95%CI 0.56 to 0.91). However, the effect of dependency in ADL on willingness to deprescribe was significantly modified by the history of CVD. One hundred five pharmacists (97%) reported to interact with physicians to clarify questions regarding prescriptions at least once a week and 88 (81%) wished to be more involved in deprescribing and medication review.
Pharmacists were willing to make deprescribing suggestions for older patients with polypharmacy, but two-thirds reported having received no formal training on how to perform structured medication reviews. Pharmacists would like to be more involved in the process of medication review and deprescribing, which should be leveraged in the context of Swiss primary care settings.
医生和药剂师之间的合作有助于开展药物优化工作。在减少用药的背景下,药剂师的角色通常被描述为向医生提出减少用药建议。在瑞士初级保健环境中,关于药剂师愿意提出减少用药建议的因素及其与医生的专业间合作,我们知之甚少。
探讨药剂师对老年人药物优化和减少用药的看法,以及他们在瑞士初级保健环境中对专业间合作的偏好。
在这项横断面研究中,瑞士药剂师协会 pharmaSuisse 的 1000 名药剂师成员被随机邀请参与一项关于药物优化、减少用药和专业间合作的调查。该调查包含三个患有多种疾病、年龄均≥80 岁、日常生活活动(ADL)和心血管疾病(CVD)依赖程度不同的多病老年患者的病例描述。对于每个病例描述,药剂师被问及他们是否会减少用药以及会减少哪些药物。我们根据病例描述计算了药剂师减少用药的意愿比例,并进行了多水平逻辑回归分析,以评估 CVD、ADL 和减少用药意愿之间的关联。
共有 138 名(14%)药剂师对调查做出了回应:113 名(82%)为女性,平均年龄为 44 岁(标准差=11),66%(n=77)报告从未接受过任何关于如何进行结构化药物审查的特定培训。83 名(72%)药剂师表示对识别减少用药机会有信心。所有药剂师在所有病例描述中均表示愿意减少≥1 种药物。患有 CVD 的患者减少用药的可能性较低(OR=0.27,95%CI 0.21 至 0.36)。ADL 依赖性越高(中重度与轻度依赖性:OR=0.68,95%CI 0.54 至 0.87,重度与轻度依赖性:OR=0.72,95%CI 0.56 至 0.91),减少用药的意愿越低。然而,ADL 依赖性对减少用药意愿的影响因 CVD 病史而显著改变。105 名(97%)药剂师报告至少每周与医生互动一次以澄清处方相关问题,88 名(81%)希望更多地参与减少用药和药物审查。
药剂师愿意为患有多种疾病且用药过多的老年患者提出减少用药建议,但三分之二的药剂师报告称他们没有接受过如何进行结构化药物审查的正式培训。药剂师希望更多地参与药物审查和减少用药的过程,这应在瑞士初级保健环境中加以利用。