Sartori Laura F, Tsemberis Elena, Hernandez Tyne, Luchette Katherine, Zhang Donglan, Farooqi Sumera, Bush Jenny, McCann John C, Balamuth Fran, Weiss Scott L
Department of Emergency Medicine, Children's Hospital of Philadelphia, Philadelphia, PA, USA.
University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA.
Pediatr Res. 2025 Feb;97(3):1127-1133. doi: 10.1038/s41390-024-03420-z. Epub 2024 Aug 3.
Mitochondrial dysfunction, linked to sepsis-related organ failure, is unknown in febrile illness.
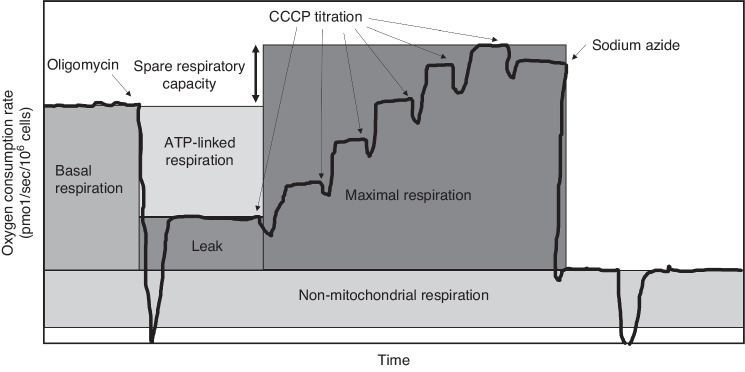
Prospective study of children in an Emergency Department (ED) with febrile illness or without infection (ED controls); secondary analysis of ICU patients with sepsis or without infection (ICU controls). Mitochondrial oxygen consumption measured in peripheral blood mononuclear cells using respirometry, with primary outcome of spare respiratory capacity (SRC). Mitochondrial content measured as citrate synthase (CS: febrile illness and ED controls) and mitochondrial to nuclear DNA ratio (mtDNA:nDNA: all groups).
SRC was lower in febrile illness (6.7 ± 3.0 pmol/sec/10 cells) and sepsis (5.7 ± 4.7) than ED/PICU controls (8.5 ± 3.7; both p < 0.05), but not different between febrile illness and sepsis (p = 0.26). Low SRC was driven by increased basal respiration in febrile illness and decreased maximal uncoupled respiration in sepsis. Differences were no longer significant after adjustment for patient demographics. Febrile illness demonstrated lower CS activity than ED controls (p = 0.07) and lower mtDNA:nDNA than both ED/PICU controls and sepsis (both p < 0.05).
Mitochondrial SRC was reduced in both febrile illness and sepsis, but due to distinct mitochondrial profiles and impacted by demographics. Further work is needed to determine if mitochondrial profiles could differentiate febrile illness from early sepsis.
Mitochondrial dysfunction has been linked to organ failure in sepsis, but whether mitochondrial alterations are evident in febrile illness without sepsis is unknown. In our study, while mitochondrial spare respiratory capacity (SRC), an index of cellular bioenergetic reserve under stress, was reduced in children with both febrile illness and sepsis compared to children without infections, low SRC was driven by increased basal respiration in febrile illness compared with decreased maximal uncoupled respiration in sepsis. Additional research is needed to understand if distinct mitochondrial profiles could be used to differentiate febrile illness from early sepsis in children.
线粒体功能障碍与脓毒症相关器官衰竭有关,在发热性疾病中尚不清楚。
对急诊科患有发热性疾病或无感染的儿童进行前瞻性研究(急诊科对照);对重症监护病房患有脓毒症或无感染的患者进行二次分析(重症监护病房对照)。使用呼吸测定法测量外周血单核细胞中的线粒体氧消耗,主要结果为备用呼吸能力(SRC)。线粒体含量以柠檬酸合酶(CS:发热性疾病和急诊科对照)和线粒体与核DNA比率(mtDNA:nDNA:所有组)来衡量。
发热性疾病(6.7±3.0 pmol/秒/10个细胞)和脓毒症(5.7±4.7)中的SRC低于急诊科/儿科重症监护病房对照(8.5±3.7;两者p<0.05),但发热性疾病和脓毒症之间无差异(p=0.26)。发热性疾病中SRC降低是由基础呼吸增加所致,脓毒症中则是由最大解偶联呼吸降低所致。在对患者人口统计学进行调整后,差异不再显著。发热性疾病的CS活性低于急诊科对照(p=0.07),mtDNA:nDNA低于急诊科/儿科重症监护病房对照和脓毒症(两者p<0.05)。
发热性疾病和脓毒症中的线粒体SRC均降低,但由于线粒体特征不同且受人口统计学影响。需要进一步研究以确定线粒体特征是否可区分发热性疾病和早期脓毒症。
线粒体功能障碍与脓毒症中的器官衰竭有关,但在无脓毒症的发热性疾病中线粒体改变是否明显尚不清楚。在我们的研究中,虽然与未感染儿童相比,发热性疾病和脓毒症儿童的线粒体备用呼吸能力(SRC)(一种应激下细胞生物能量储备指标)降低,但发热性疾病中SRC降低是由基础呼吸增加所致,而脓毒症中是由最大解偶联呼吸降低所致。需要更多研究来了解不同的线粒体特征是否可用于区分儿童发热性疾病和早期脓毒症。