Butnariu Andreea D, Miron Ioana, David Bogdan, Visarion Dan M, Pruna Violeta I, Pruna Viorel M
Neurosurgery Department, Bagdasar-Arseni Clinical Emergency Hospital, Bucharest, ROU.
Neurosurgery Department, Carol Davila University of Medicine and Pharmacy, Bucharest, ROU.
Cureus. 2024 Jul 4;16(7):e63846. doi: 10.7759/cureus.63846. eCollection 2024 Jul.
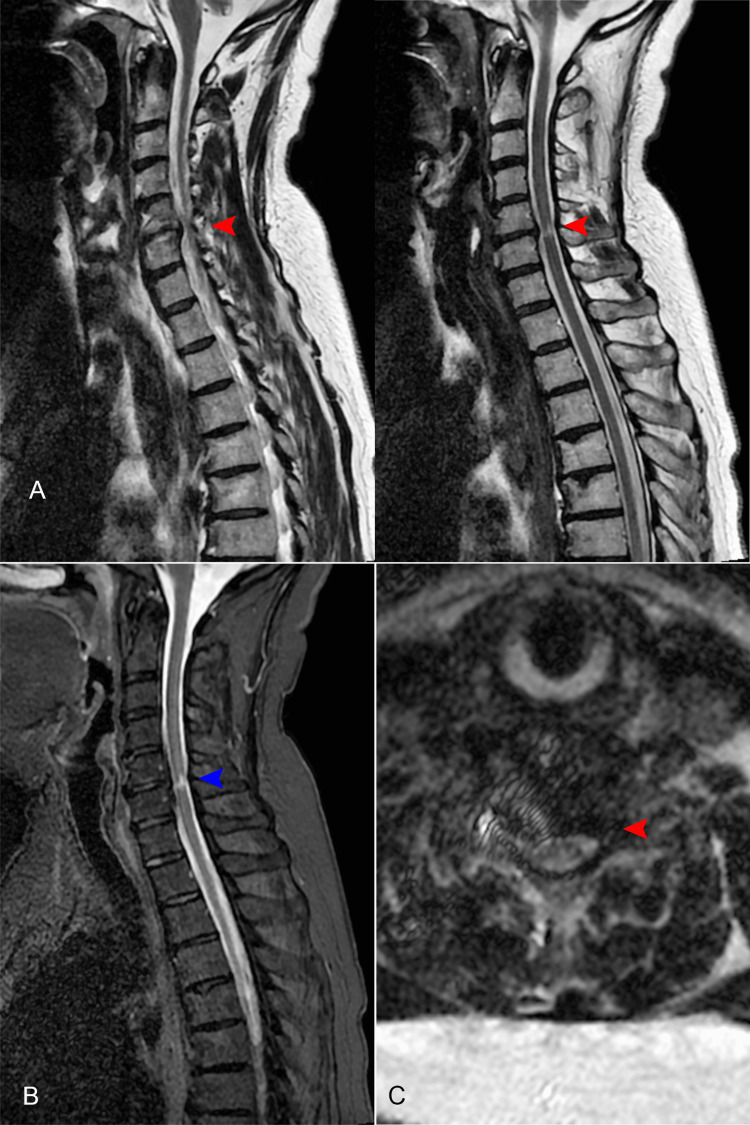
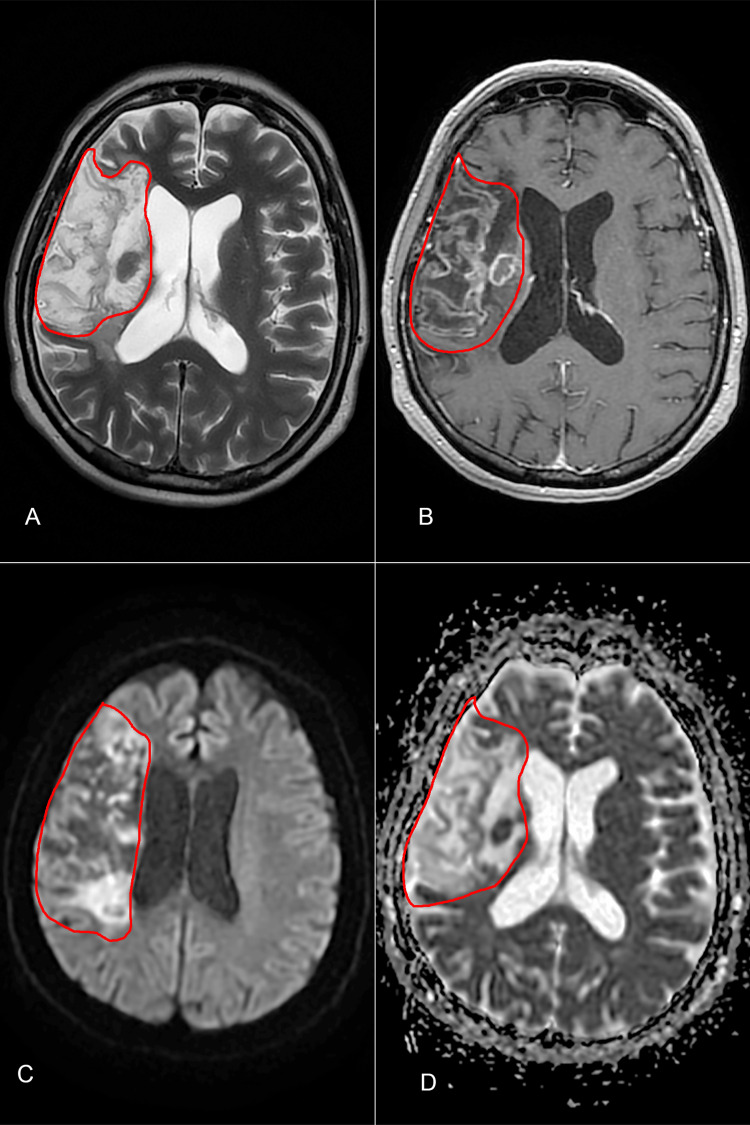
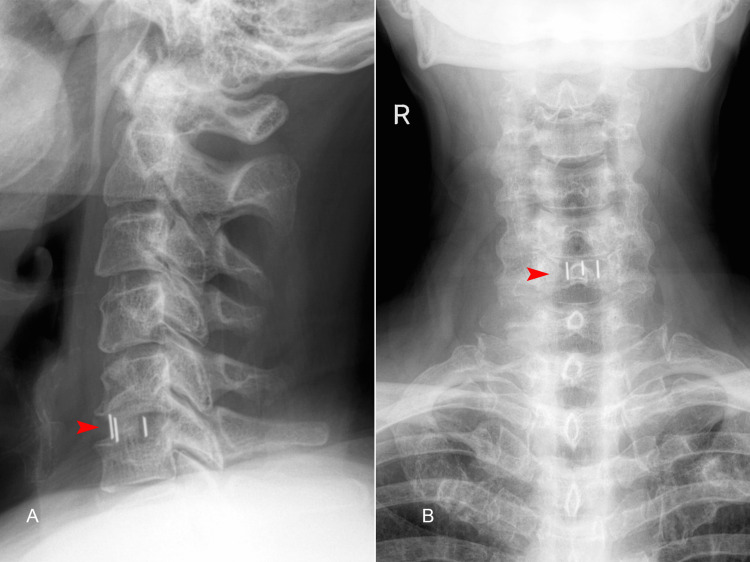
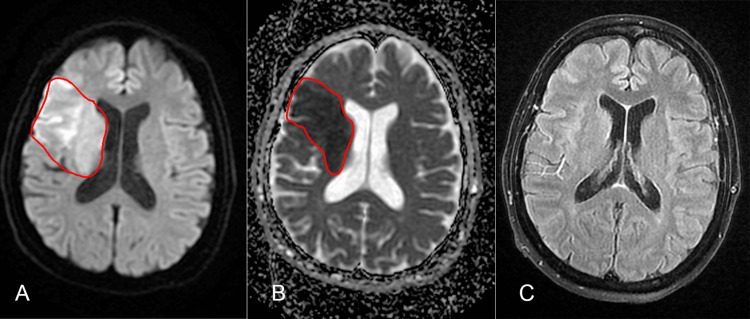
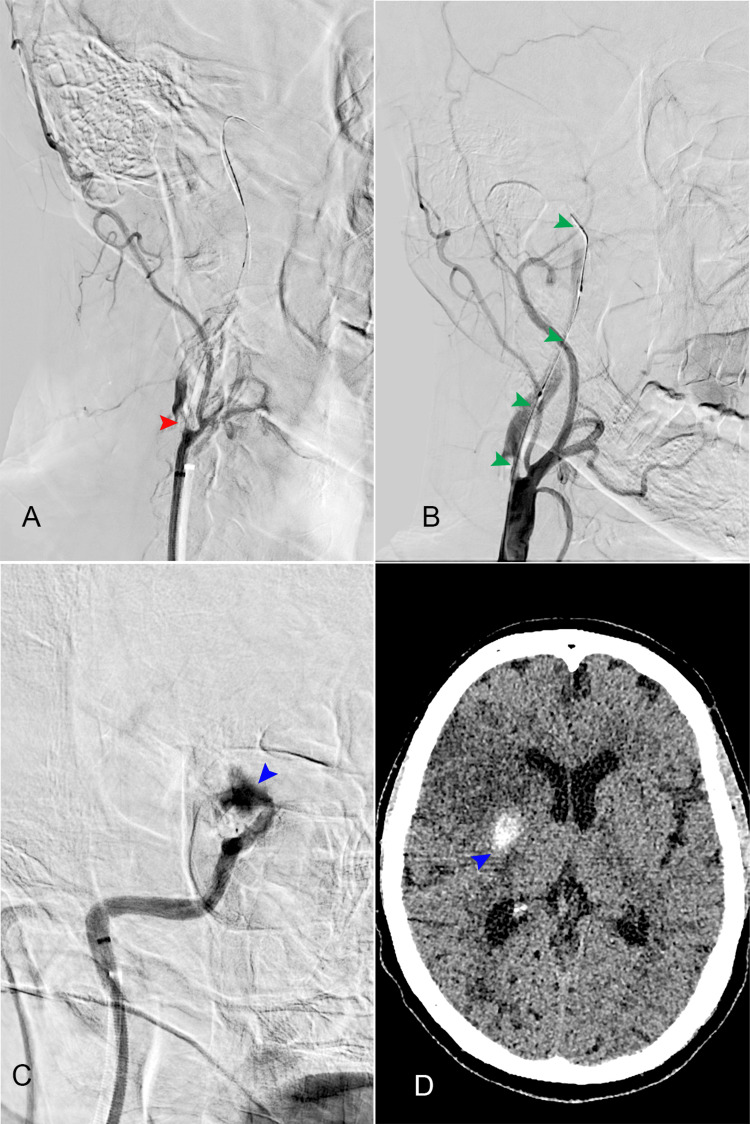
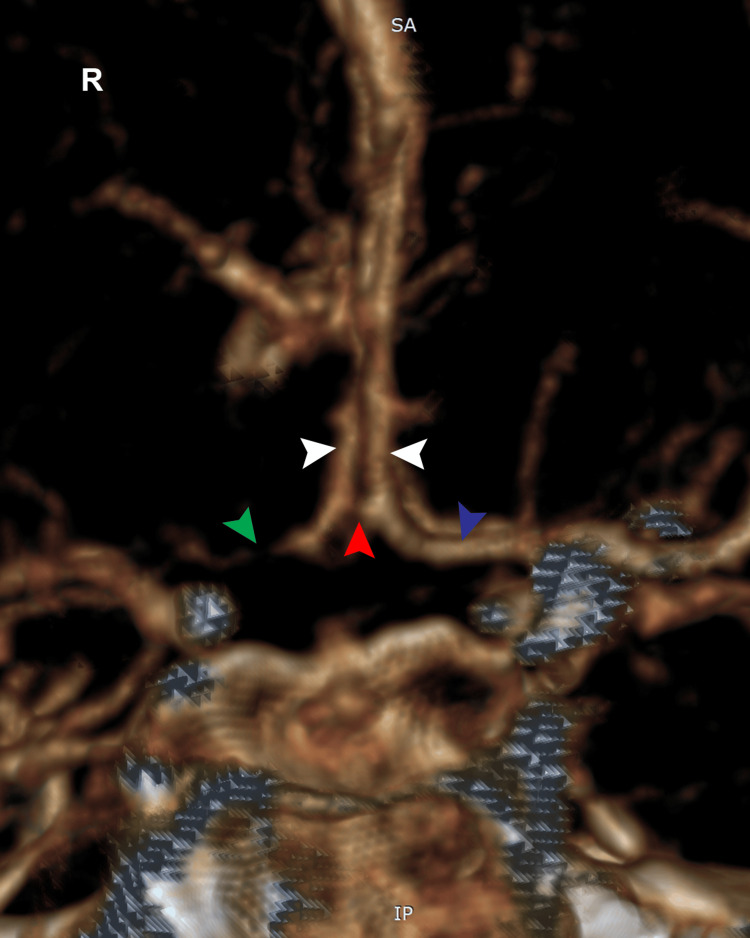
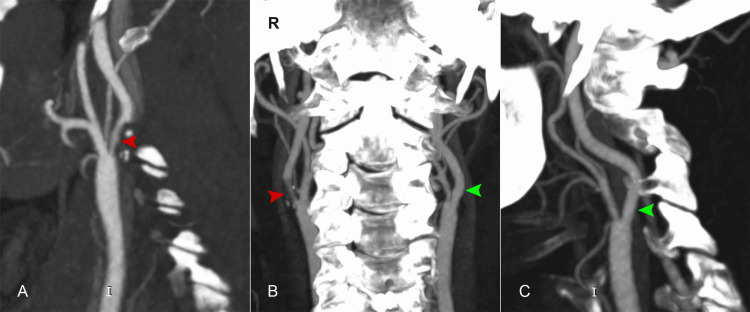
Vascular complications succeeding anterior cervical spine surgery are rare, but their consequences represent a major burden for the patient. Cerebral infarction following anterior cervical discectomy and fusion (ACDF) is uncommon. However, screening for risk factors before surgery should become mandatory. We present the case of a patient with no significant medical history who underwent ACDF for a C5/C6 herniated disc with myelopathy. Although the surgery was uneventful, after the surgery, partial right palpebral ptosis and miosis were noted, suggestive of Horner syndrome. On the fifth postoperative day, the patient experienced left hemiplegia and drowsiness. An emergency CT scan and cerebral MRI revealed ischemia in the right middle cerebral artery territory. The patient was transferred to a neurology center for mechanical thrombectomy, which revealed a complete occlusion of the right internal carotid artery. The procedure had to be halted due to blood extravasation at the internal carotid artery bifurcation to prevent further complications. An angio-CT examination of the cervical arteries exposed a soft atheromatous plaque on the right internal carotid artery, immediately after the bifurcation. Despite the patient having no significant medical history, blood tests indicated dyslipidemia. At the two-month follow-up, the patient remained hemiplegic, with mild dysphasia. Performing carotid and vertebral Doppler ultrasound before cervical spine surgery might be useful, whenever possible, to assess high-risk factors for ischemic events and avoid such debilitating complications.
颈椎前路手术后发生的血管并发症很少见,但其后果给患者带来了重大负担。颈椎前路椎间盘切除融合术(ACDF)后发生脑梗死并不常见。然而,术前筛查危险因素应成为常规操作。我们报告一例患者,该患者无重大病史,因C5/C6椎间盘突出伴脊髓病接受了ACDF手术。尽管手术过程顺利,但术后发现患者出现右侧上睑轻度下垂和瞳孔缩小,提示霍纳综合征。术后第5天,患者出现左侧偏瘫和嗜睡。急诊CT扫描和脑部MRI显示右侧大脑中动脉供血区缺血。患者被转至神经科中心进行机械取栓术,结果显示右侧颈内动脉完全闭塞。由于颈内动脉分叉处出血,为防止进一步并发症,手术不得不中止。颈部动脉血管CT检查显示右侧颈内动脉在分叉后 immediately 处有一个软斑块。尽管患者无重大病史,但血液检查显示血脂异常。在两个月的随访中,患者仍偏瘫,伴有轻度失语。只要有可能,在颈椎手术前进行颈动脉和椎动脉多普勒超声检查可能有助于评估缺血事件的高危因素,避免此类使人衰弱的并发症。