Department of Otorhinolaryngology-Head and Neck Surgery, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Corporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, Pennsylvania, USA.
Otolaryngol Head Neck Surg. 2024 Dec;171(6):1705-1714. doi: 10.1002/ohn.928. Epub 2024 Aug 5.
Mandibular plate reconstruction (MPR) is often indicated after tumor ablation, osteoradionecrosis excision, and traumatic bone loss to restore oral functionality and facial cosmetics. There are limited analyses identifying risk factors that lead to plate infection (PIn), exposure, and removal ("plate complications").
Retrospective cohort study.
Academic tertiary medical center.
Patients who underwent MPR from 2013 to 2022 were identified. Risk factors for plate complications were analyzed based on demographic, clinical, intraoperative, and postoperative factors. Multivariable analysis was conducted with logistic regression. Survival analysis was conducted with a Cox model.
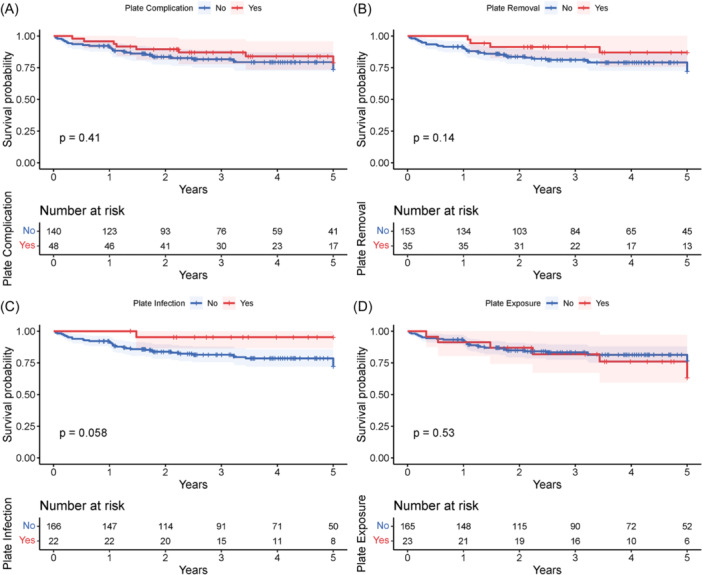
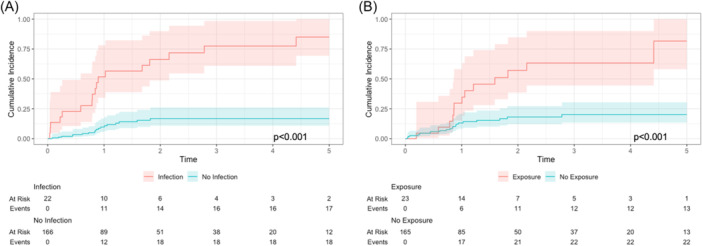
Of the 188 patients analyzed, 48 (25.5%) had a plate complication [infection: 22 (11.7%); exposure: 23 (12.2%); removal: 35 (18.6%)]. Multivariate analysis revealed predictive associations between at least 1 plate complication and the following variables: smoking status, soft tissue defect size, number of plates, average screw length, and various postoperative complications. Other associations approached the threshold for significance. Prior and adjuvant radiation therapy, type of free flap, stock versus custom plates, and perioperative antibiotic prophylaxis regimens were not associated with plate complications. No plate complication was independently associated with lower overall survival. PIn (hazard ratio, HR: 7.99, confidence interval, CI [4.11, 15.54]) and exposure (HR: 3.56, CI [1.79, 7.08]) were independently associated with higher rates of plate removal.
Plate complications are relatively common after MPR. Smoking history, specific disease characteristics, hardware used during surgery, and postoperative complications may help identify higher-risk patients, but additional larger-scale studies are needed to validate our findings and resolve discrepancies in the current literature.
下颌骨板重建(MPR)常用于肿瘤消融、骨放射性坏死切除和外伤性骨缺失后,以恢复口腔功能和面部美观。目前已有一些有限的分析确定了导致钢板感染(PIn)、暴露和移除(“钢板并发症”)的危险因素。
回顾性队列研究。
学术性三级医疗中心。
确定了 2013 年至 2022 年间接受 MPR 的患者。根据人口统计学、临床、手术中和术后因素分析了钢板并发症的危险因素。采用逻辑回归进行多变量分析。采用 Cox 模型进行生存分析。
在 188 例患者中,有 48 例(25.5%)发生了钢板并发症[感染:22 例(11.7%);暴露:23 例(12.2%);移除:35 例(18.6%)]。多变量分析显示,至少有一种钢板并发症与以下变量之间存在预测性关联:吸烟状况、软组织缺损大小、钢板数量、平均螺钉长度和各种术后并发症。其他关联接近显著水平。既往和辅助放疗、游离皮瓣类型、库存与定制钢板以及围手术期抗生素预防方案与钢板并发症无关。没有钢板并发症与总体生存率降低独立相关。PIn(风险比,HR:7.99,置信区间,CI [4.11,15.54])和暴露(HR:3.56,CI [1.79,7.08])与更高的钢板移除率独立相关。
MPR 后钢板并发症较为常见。吸烟史、特定疾病特征、手术中使用的硬件以及术后并发症可能有助于识别高风险患者,但需要进一步开展更大规模的研究来验证我们的发现,并解决当前文献中的差异。