Sidler Fabian, Turcan Vitalie, Storni Federico, Bernhard Sarah, Jakob Dominik A, Ehrhard Simone
Department of General Internal Medicine Inselspital Bern University Hospital University of Bern, Bern, Switzerland.
Department of Visceral Surgery and Medicine Inselspital Bern University Hospital University of Bern, Bern, Switzerland.
Case Reports Hepatol. 2024 Jul 29;2024:7921410. doi: 10.1155/2024/7921410. eCollection 2024.
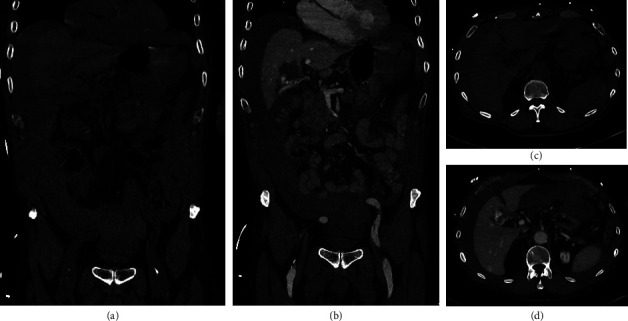
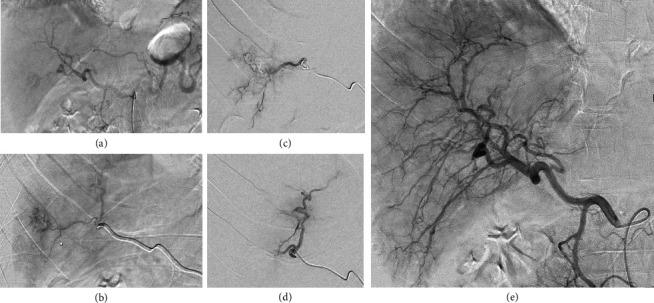
Syncope is common in emergency medicine, but only a minority of syncopes is caused by hemorrhage. Liver hemangioma is the most frequent benign liver tumor, and they rarely lead to symptoms or complications. . We describe the case of an 81-year-old man with hemorrhagic shock due to an atraumatic rupture of a hepatic hemangioma while on oral anticoagulation. The patient presented to the emergency department after three episodes of syncope before admission, nausea, vomiting, mild epigastric abdominal pain, but with clinical signs of peritonitis. On admission, the patient had a mild tachycardia with a heart rate of 107/min and a blood pressure of 102/83 mmHg. Initial hemoglobin was 122 g/L, and lactate was slightly elevated (2.5 mmol/L). Bedside sonography revealed free intraabdominal fluid. The subsequent computed tomography showed a ruptured hemangioma of the liver with ongoing hemorrhage. After the CT scan, the patient became increasingly tachycardic and the blood pressure dropped to 94/62 mmHg. After administration of blood products and intravenous fluids, the patient responded with improved hemodynamics and was transferred to angiology for emergency embolization. After the intervention, the patient spent two days in the intermediate care unit and was discharged after 10 days of hospitalization.
Atraumatic rupture of a hemangioma with consecutive hemorrhagic shock is extremely rare. In selected cases of spontaneously ruptured hemangiomas with hemoperitoneum, endovascular embolization can be an alternative to surgery. Furthermore, this case emphasizes the importance of sonographic examination as an additional diagnostic tool in syncope and concomitant abdominal pain.
晕厥在急诊医学中很常见,但只有少数晕厥是由出血引起的。肝血管瘤是最常见的肝脏良性肿瘤,很少导致症状或并发症。我们描述了一例81岁男性患者,在口服抗凝剂期间因肝血管瘤非创伤性破裂导致失血性休克。患者在入院前发生三次晕厥、恶心、呕吐、轻度上腹部腹痛后就诊于急诊科,但有腹膜炎的临床体征。入院时,患者轻度心动过速,心率为107次/分钟,血压为102/83 mmHg。初始血红蛋白为122 g/L,乳酸略有升高(2.5 mmol/L)。床边超声检查发现腹腔内有游离液体。随后的计算机断层扫描显示肝脏血管瘤破裂并持续出血。CT扫描后,患者心动过速加剧,血压降至94/62 mmHg。在输注血液制品和静脉输液后,患者血流动力学得到改善,并被转至血管病科进行紧急栓塞治疗。介入治疗后,患者在中间护理病房住了两天,住院10天后出院。
血管瘤非创伤性破裂并连续发生失血性休克极为罕见。在某些自发性肝血管瘤破裂并伴有血腹的病例中,血管内栓塞可作为手术的替代方法。此外,该病例强调了超声检查作为晕厥和伴发腹痛的辅助诊断工具的重要性。