Tang Hao-Huan, Zhou Lin-Feng, Wang Chun-Xin, Zha Yang, Fan Chen, Zhong Bin-Yan, Zhu Xiao-Li, Wang Wei-Dong
Department of Interventional Radiology, The Affiliated Wuxi People's Hospital of Nanjing Medical University, Wuxi People's Hospital, Wuxi Medical Center, Nanjing Medical University, Wuxi, 214023, People's Republic of China.
Department of Interventional Radiology, The First Affiliated Hospital of Soochow University, Suzhou, 215006, People's Republic of China.
J Inflamm Res. 2024 Aug 1;17:5211-5221. doi: 10.2147/JIR.S467583. eCollection 2024.
The objective of this study was to investigate the effect of neutrophil-to-lymphocyte ratio (NLR) on the survival of cirrhotic patients with esophagogastric variceal bleeding (EGVB) treated with transjugular intrahepatic portosystemic shunt (TIPS).
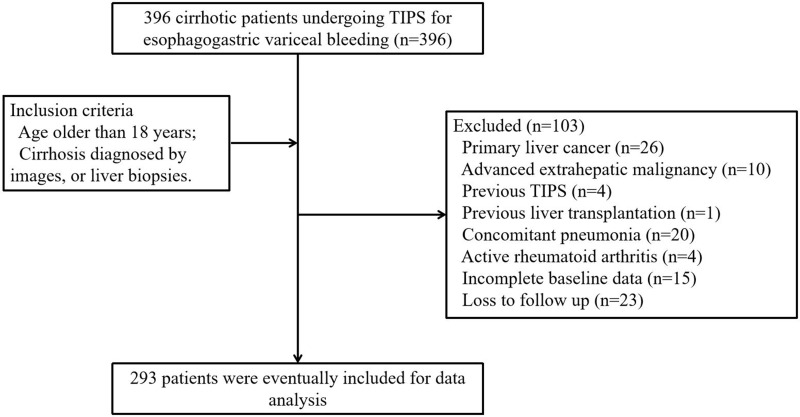
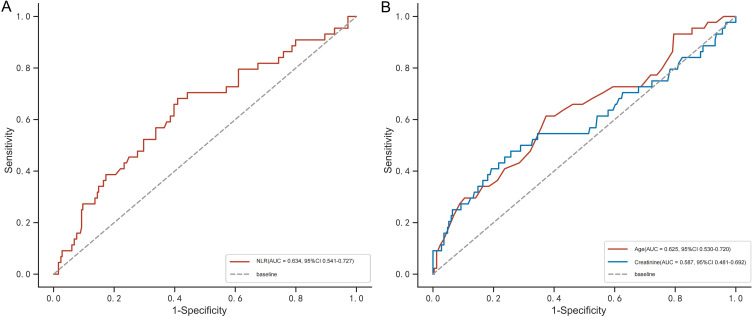
A total of 293 patients treated with TIPS were included. The receiver operator characteristic curve (ROC) was used to calculate the optimal cut-off values of parameters such as NLR. The Kaplan-Meier curve and Cox proportional risk model were used to evaluate the effects of NLR and other variables on 2-year all-cause mortality.
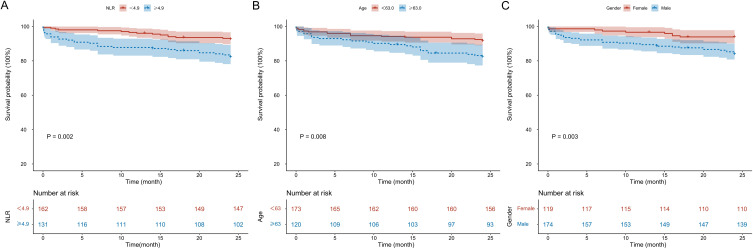
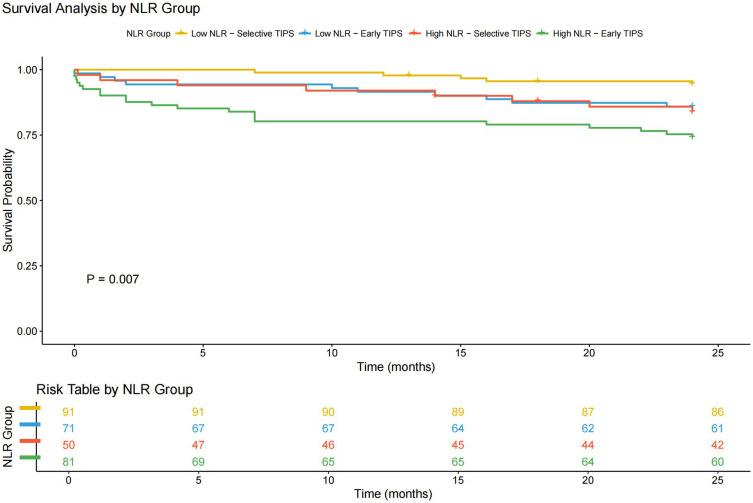
The area under the ROC for NLR was 0.634, with an optimal cutoff value of 4.9. Two-year mortality rates for patients with high (≥4.9) and low (<4.9) NLR were 22.1% and 9.3%, respectively (Log rank test: P = 0.002). After correcting for confounders, multivariate analysis demonstrated that NLR ≥ 4.9 (HR = 2.741, 95% CI 1.467-5.121, P = 0.002), age ≥ 63 (HR = 3.403, 95% CI 1.835-6.310, P < 0.001), and gender (male) (HR = 2.842, 95% CI 1.366-5.912, P = 0.001) were independent risk factors for the mortality outcome. Considering the stratification of early and selective TIPS treatment, high NLR still significantly increased the risk of mortality for patients (Log rank test: P = 0.007, HR = 2.317, 95% CI 1.232-4.356).
NLR can help to predict survival in EGVB patients after TIPS, and the type of TIPS should also be considered in practical applications.
本研究旨在探讨中性粒细胞与淋巴细胞比值(NLR)对经颈静脉肝内门体分流术(TIPS)治疗的食管胃静脉曲张破裂出血(EGVB)肝硬化患者生存情况的影响。
共纳入293例行TIPS治疗的患者。采用受试者工作特征曲线(ROC)计算NLR等参数的最佳截断值。使用Kaplan-Meier曲线和Cox比例风险模型评估NLR及其他变量对2年全因死亡率的影响。
NLR的ROC曲线下面积为0.634,最佳截断值为4.9。NLR高(≥4.9)和低(<4.9)的患者2年死亡率分别为22.1%和9.3%(对数秩检验:P = 0.002)。校正混杂因素后,多因素分析表明NLR≥4.9(HR = 2.741,95%CI 1.467 - 5.121,P = 0.002)、年龄≥63岁(HR = 3.403,95%CI 1.835 - 6.310,P < 0.001)和性别(男性)(HR = 2.842,95%CI 1.366 - 5.912,P = 0.001)是死亡结局的独立危险因素。考虑早期和选择性TIPS治疗的分层情况,高NLR仍显著增加患者的死亡风险(对数秩检验:P = 0.007,HR = 2.317,95%CI 1.232 - 4.356)。
NLR有助于预测TIPS术后EGVB患者的生存情况,在实际应用中还应考虑TIPS的类型。