Sf Nectarie Oncology Center and University of Medicine and Pharmacy, Craiova, Romania.
Bradford Hill Clinical Research Center, Santiago, Chile.
J Immunother Cancer. 2024 Aug 6;12(8):e008872. doi: 10.1136/jitc-2024-008872.
Checkpoint inhibitor therapy has demonstrated overall survival benefit in multiple tumor types. Tumor mutational burden (TMB) is a predictive biomarker for response to immunotherapies. This study evaluated the efficacy of nivolumab+ipilimumab in multiple tumor types based on TMB status evaluated using either tumor tissue (tTMB) or circulating tumor DNA in the blood (bTMB).
Patients with metastatic or unresectable solid tumors with high (≥10 mutations per megabase) tTMB (tTMB-H) and/or bTMB (bTMB-H) who were refractory to standard therapies were randomized 2:1 to receive nivolumab+ipilimumab or nivolumab monotherapy in an open-label, phase 2 study (CheckMate 848; NCT03668119). tTMB and bTMB were determined by the Foundation Medicine FoundationOne CDx test and bTMB Clinical Trial Assay, respectively. The dual primary endpoints were objective response rate (ORR) in patients with tTMB-H and/or bTMB-H tumors treated with nivolumab+ipilimumab.
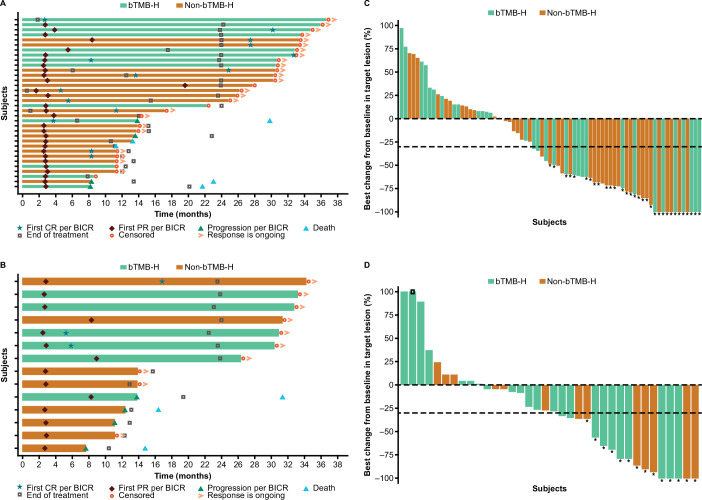
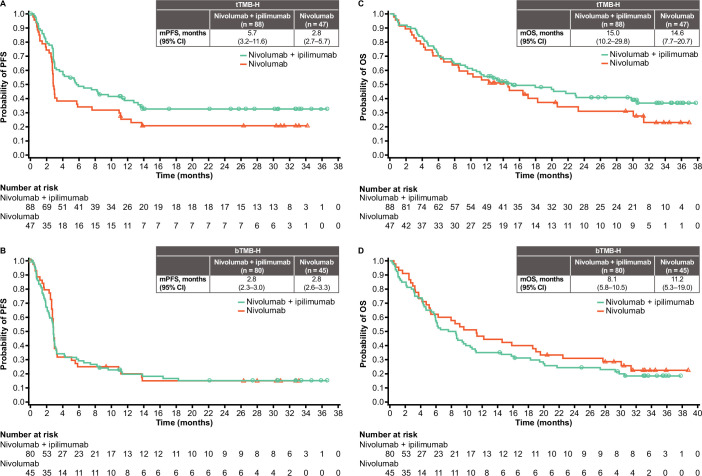
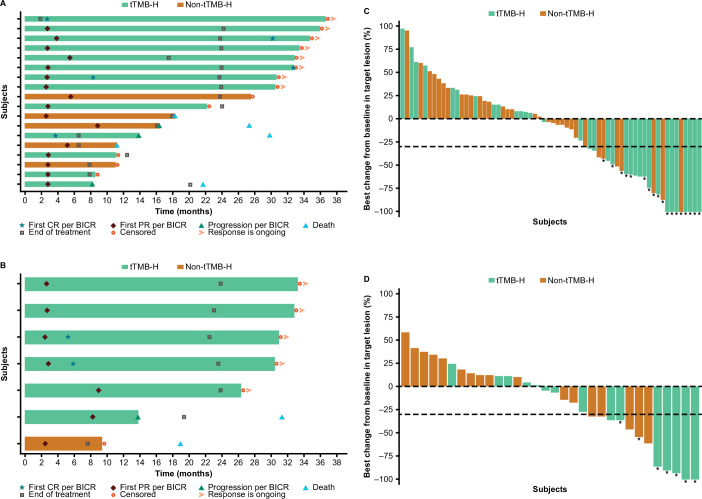
In total, 201 patients refractory to standard therapies were randomized: 135 had tTMB-H and 125 had bTMB-H; 82 patients had dual tTMB-H/bTMB-H. In patients with tTMB-H, ORR was 38.6% (95% CI 28.4% to 49.6%) with nivolumab+ipilimumab and 29.8% (95% CI 17.3% to 44.9%) with nivolumab monotherapy. In patients with bTMB-H, ORR was 22.5% (95% CI 13.9% to 33.2%) with nivolumab+ipilimumab and 15.6% (95% CI 6.5% to 29.5%) with nivolumab monotherapy. Early and durable responses to treatment with nivolumab+ipilimumab were seen in patients with tTMB-H or bTMB-H. The safety profile of nivolumab+ipilimumab was manageable, with no new safety signals.
Patients with metastatic or unresectable solid tumors with TMB-H, as determined by tissue biopsy or by blood sample when tissue biopsy is unavailable, who have no other treatment options, may benefit from nivolumab+ipilimumab.
NCT03668119.
检查点抑制剂疗法在多种肿瘤类型中显示出总生存获益。肿瘤突变负担(TMB)是免疫治疗反应的预测生物标志物。本研究根据使用肿瘤组织(tTMB)或血液中的循环肿瘤 DNA(bTMB)评估的 TMB 状态,评估了纳武利尤单抗+伊匹单抗在多种肿瘤类型中的疗效。
患有转移性或不可切除的固体肿瘤且对标准治疗耐药的患者,TMB 高(≥10 个每兆碱基突变)(tTMB-H)和/或 bTMB(bTMB-H),随机接受纳武利尤单抗+伊匹单抗或纳武利尤单抗单药治疗,分组比例为 2:1,这是一项开放标签、2 期研究(CheckMate 848;NCT03668119)。tTMB 和 bTMB 分别由 Foundation Medicine FoundationOne CDx 检测和 bTMB 临床试验检测确定。主要双重终点是接受纳武利尤单抗+伊匹单抗治疗的 tTMB-H 和/或 bTMB-H 肿瘤患者的客观缓解率(ORR)。
共有 201 名对标准治疗耐药的患者被随机分组:135 名患者 tTMB-H,125 名患者 bTMB-H;82 名患者同时存在 tTMB-H 和 bTMB-H。在 tTMB-H 患者中,纳武利尤单抗+伊匹单抗治疗的 ORR 为 38.6%(95%CI 28.4%至 49.6%),纳武利尤单抗单药治疗的 ORR 为 29.8%(95%CI 17.3%至 44.9%)。在 bTMB-H 患者中,纳武利尤单抗+伊匹单抗治疗的 ORR 为 22.5%(95%CI 13.9%至 33.2%),纳武利尤单抗单药治疗的 ORR 为 15.6%(95%CI 6.5%至 29.5%)。在 tTMB-H 或 bTMB-H 患者中,纳武利尤单抗+伊匹单抗治疗可早期和持久地缓解。纳武利尤单抗+伊匹单抗的安全性特征可管理,无新的安全性信号。
对于 TMB-H 的转移性或不可切除的实体瘤患者,无论组织活检是否可用,均可以通过组织活检或血液样本来确定 TMB-H,且这些患者没有其他治疗选择,他们可能从纳武利尤单抗+伊匹单抗治疗中获益。
NCT03668119。