Khoo Michelle Shi Qing, Koh Frederick H, Sivarajah Sharmini Su, Ho Leonard Ming-Li, Aw Darius Kang-Lie, Chong Cheryl Xi-Zi, Foo Fung Joon, Tan Winson Jianhong
Colorectal Service, Department of General Surgery, Sengkang General Hospital, Singapore.
Ann Coloproctol. 2024 Dec;40(6):555-563. doi: 10.3393/ac.2023.00738.0105. Epub 2024 Aug 5.
In patients with acute left-sided colonic obstruction, stenting can convert an emergency operation into a semi-elective procedure. However, its use continues to be debated. We performed a cost-effective analysis using our institution's experiences.
Endoscopic, surgical, and financial details were prospectively collected for patients who presented with acute colonic obstruction and underwent stenting between 2019 and 2022. Outcomes were defined as technical/clinical success and successful surgical resection. The financial cost of stenting was compared with the expected cost without stenting.
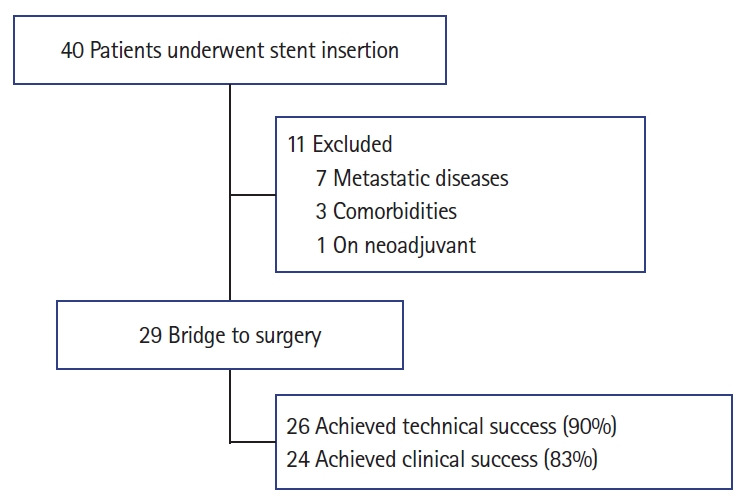
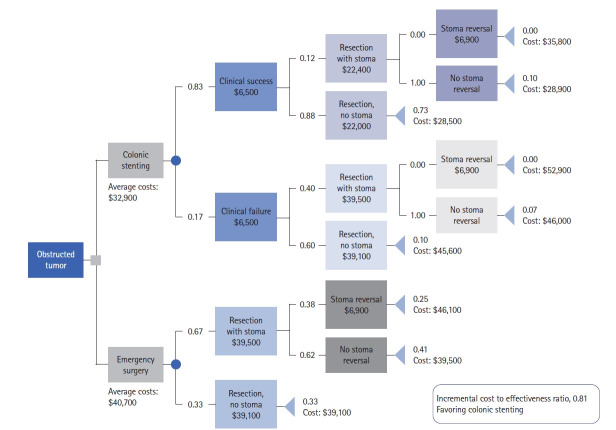
Forty patients were included, with 29 undergoing definitive resection. The most common pathology was primary colon cancer (27 patients, 93%). Endoscopic stenting had high technical (90%) and clinical (83%) success rates, with low rates of complications such as perforation (2 patients, 7%) and migration (0 patients, 0%). As a bridge to surgery, the median procedure time was 226 minutes and the surgical outcomes also showed a low rate of complications (3 patients, 11%), such as anastomotic leakage (0 patients, 0%), intraabdominal abscesses (2 patients, 7%), and 30-day postoperative mortality (0 patients, 0%). The cumulative costs with colonic stenting were $32,900, while the expected costs with emergency surgery, including stoma reversal, were $40,700 (healthcare cost-savings of $7,800 per person). The difference was mainly due to the avoidance of upfront emergency surgery. The incremental cost-effectiveness ratio was 0.81, favoring colonic stenting over upfront emergency surgery.
Colonic stenting as a bridge to surgery is safe and cost-effective for treating left-sided colonic obstruction with high success rates and low complication rates.
对于急性左侧结肠梗阻患者,支架置入术可将急诊手术转变为半择期手术。然而,其应用仍存在争议。我们利用本机构的经验进行了成本效益分析。
前瞻性收集2019年至2022年间出现急性结肠梗阻并接受支架置入术患者的内镜、手术及财务细节。结果定义为技术/临床成功和成功的手术切除。将支架置入术的财务成本与未进行支架置入术的预期成本进行比较。
纳入40例患者,其中29例接受了根治性切除。最常见的病理类型是原发性结肠癌(27例,93%)。内镜下支架置入术具有较高的技术成功率(90%)和临床成功率(83%),穿孔(2例,7%)和移位(0例,0%)等并发症发生率较低。作为手术桥梁,中位手术时间为226分钟,手术结果也显示并发症发生率较低(3例,11%),如吻合口漏(0例,0%)、腹腔内脓肿(2例,7%)和术后30天死亡率(0例,0%)。结肠支架置入术的累计成本为32,900美元,而包括造口回纳在内的急诊手术预期成本为40,700美元(人均节省医疗费用7,800美元)。差异主要是由于避免了前期的急诊手术。增量成本效益比为0.81,表明结肠支架置入术优于前期急诊手术。
结肠支架置入术作为手术桥梁治疗左侧结肠梗阻安全且具有成本效益,成功率高且并发症发生率低。