Chiarini Giovanni, Mariani Silvia, Schaefer Anne-Kristin, van Bussel Bas C T, Di Mauro Michele, Wiedemann Dominik, Saeed Diyar, Pozzi Matteo, Botta Luca, Boeken Udo, Samalavicius Robertas, Bounader Karl, Hou Xiaotong, Bunge Jeroen J H, Buscher Hergen, Salazar Leonardo, Meyns Bart, Herr Daniel, Matteucci Sacha, Sponga Sandro, Ramanathan Kollengode, Russo Claudio, Formica Francesco, Sakiyalak Pranya, Fiore Antonio, Camboni Daniele, Raffa Giuseppe Maria, Diaz Rodrigo, Wang I-Wen, Jung Jae-Seung, Belohlavek Jan, Pellegrino Vin, Bianchi Giacomo, Pettinari Matteo, Barbone Alessandro, Garcia José P, Shekar Kiran, Whitman Glenn J R, Lorusso Roberto
Cardio-Thoracic Surgery Department, Cardiovascular Research Institute Maastricht, Maastricht University Medical Centre, P. Debyelaan, 25-6202AZ, Maastricht, The Netherlands.
Intensive Care Unit, Spedali Civili University Hospital, Brescia, Italy.
Crit Care. 2024 Aug 7;28(1):265. doi: 10.1186/s13054-024-05047-2.
Cerebral perfusion may change depending on arterial cannulation site and may affect the incidence of neurologic adverse events in post-cardiotomy extracorporeal life support (ECLS). The current study compares patients' neurologic outcomes with three commonly used arterial cannulation strategies (aortic vs. subclavian/axillary vs. femoral artery) to evaluate if each ECLS configuration is associated with different rates of neurologic complications.
This retrospective, multicenter (34 centers), observational study included adults requiring post-cardiotomy ECLS between January 2000 and December 2020 present in the Post-Cardiotomy Extracorporeal Life Support (PELS) Study database. Patients with Aortic, Subclavian/Axillary and Femoral cannulation were compared on the incidence of a composite neurological end-point (ischemic stroke, cerebral hemorrhage, brain edema). Secondary outcomes were overall in-hospital mortality, neurologic complications as cause of in-hospital death, and post-operative minor neurologic complications (seizures). Association between cannulation and neurological outcomes were investigated through linear mixed-effects models.
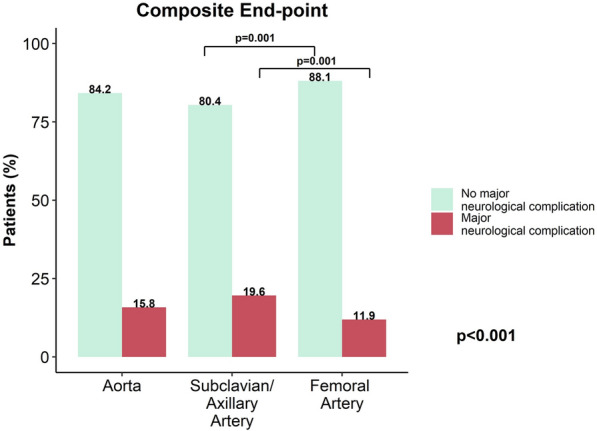
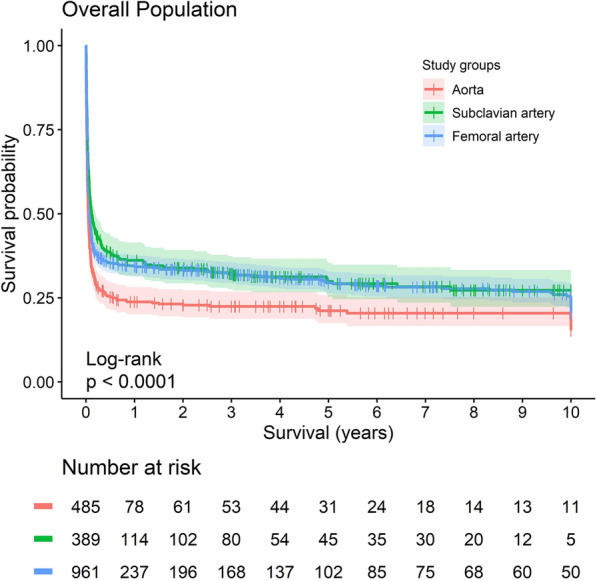
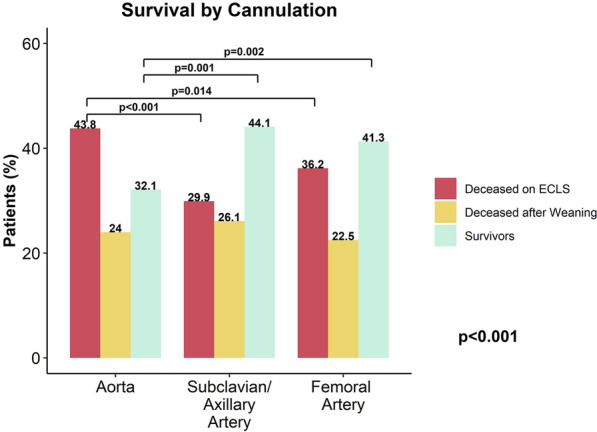
This study included 1897 patients comprising 26.5% Aortic (n = 503), 20.9% Subclavian/Axillary (n = 397) and 52.6% Femoral (n = 997) cannulations. The Subclavian/Axillary group featured a more frequent history of hypertension, smoking, diabetes, previous myocardial infarction, dialysis, peripheral artery disease and previous stroke. Neuro-monitoring was used infrequently in all groups. Major neurologic complications were more frequent in Subclavian/Axillary (Aortic: n = 79, 15.8%; Subclavian/Axillary: n = 78, 19.6%; Femoral: n = 118, 11.9%; p < 0.001) also after mixed-effects model adjustment (OR 1.53 [95% CI 1.02-2.31], p = 0.041). Seizures were more common in Subclavian/Axillary (n = 13, 3.4%) than Aortic (n = 9, 1.8%) and Femoral cannulation (n = 12, 1.3%, p = 0.036). In-hospital mortality was higher after Aortic cannulation (Aortic: n = 344, 68.4%, Subclavian/Axillary: n = 223, 56.2%, Femoral: n = 587, 58.9%, p < 0.001), as shown by Kaplan-Meier curves. Anyhow, neurologic cause of death (Aortic: n = 12, 3.9%, Subclavian/Axillary: n = 14, 6.6%, Femoral: n = 28, 5.0%, p = 0.433) was similar.
In this analysis of the PELS Study, Subclavian/Axillary cannulation was associated with higher rates of major neurologic complications and seizures. In-hospital mortality was higher after Aortic cannulation, despite no significant differences in incidence of neurological cause of death in these patients. These results encourage vigilance for neurologic complications and neuromonitoring use in patients on ECLS, especially with Subclavian/Axillary cannulation.
脑灌注可能因动脉插管部位而异,并可能影响心脏术后体外生命支持(ECLS)中神经不良事件的发生率。本研究比较了患者采用三种常用动脉插管策略(主动脉插管与锁骨下/腋动脉插管与股动脉插管)后的神经学结局,以评估每种ECLS配置是否与不同的神经并发症发生率相关。
这项回顾性、多中心(34个中心)的观察性研究纳入了2000年1月至2020年12月期间在心脏术后体外生命支持(PELS)研究数据库中接受心脏术后ECLS的成年人。比较了采用主动脉、锁骨下/腋动脉和股动脉插管的患者发生复合神经终点事件(缺血性卒中、脑出血、脑水肿)的发生率。次要结局包括总体住院死亡率、作为住院死亡原因的神经并发症以及术后轻微神经并发症(癫痫发作)。通过线性混合效应模型研究插管与神经学结局之间的关联。
本研究纳入了1897例患者,其中26.5%采用主动脉插管(n = 503),20.9%采用锁骨下/腋动脉插管(n = 397),52.6%采用股动脉插管(n = 997)。锁骨下/腋动脉组患者的高血压、吸烟、糖尿病、既往心肌梗死、透析、外周动脉疾病和既往卒中病史更为常见。所有组中神经监测的使用频率均较低。锁骨下/腋动脉组的主要神经并发症更为常见(主动脉插管组:n = 79,15.8%;锁骨下/腋动脉组:n = 78,19.6%;股动脉组:n = 118,11.9%;p < 0.001),在混合效应模型调整后也是如此(OR 1.53 [95% CI 1.02 - 2.31],p = 0.041)。锁骨下/腋动脉组的癫痫发作比主动脉插管组(n = 9,1.8%)和股动脉插管组(n = 12,1.3%)更常见(p = 0.036)。主动脉插管后的住院死亡率更高(主动脉插管组:n = 344,68.4%;锁骨下/腋动脉组:n = 223,56.2%;股动脉组:n = 587,58.9%;p < 0.001),Kaplan - Meier曲线显示了这一点。然而,神经源性死亡原因(主动脉插管组:n = 12,3.9%;锁骨下/腋动脉组:n = 14,6.6%;股动脉组:n = 28,5.0%;p = 0.433)相似。
在对PELS研究的这项分析中,锁骨下/腋动脉插管与较高的主要神经并发症和癫痫发作发生率相关。主动脉插管后的住院死亡率更高,尽管这些患者的神经源性死亡发生率没有显著差异。这些结果促使人们对接受ECLS的患者,尤其是采用锁骨下/腋动脉插管的患者的神经并发症和神经监测使用保持警惕。