Hernandez Alexandra E, Meece Matthew, Benck Kelley, Bello Gianna, Huerta Carlos Theodore, Collie Brianna L, Nguyen Jennifer, Paluvoi Nivedh
Department of Surgery, University of Miami Health System, Miami, FL 33136, USA.
DeWitt Daughtry Family Department of Surgery, Jackson Health System, Miami, FL 33136, USA.
Healthcare (Basel). 2024 Jul 30;12(15):1513. doi: 10.3390/healthcare12151513.
Combined pre-operative bowel preparation with oral antibiotics (OAB) and mechanical bowel preparation (MBP) is the current recommendation for elective colorectal surgery. Few have studied racial disparities in bowel preparation and subsequent post-operative complications.
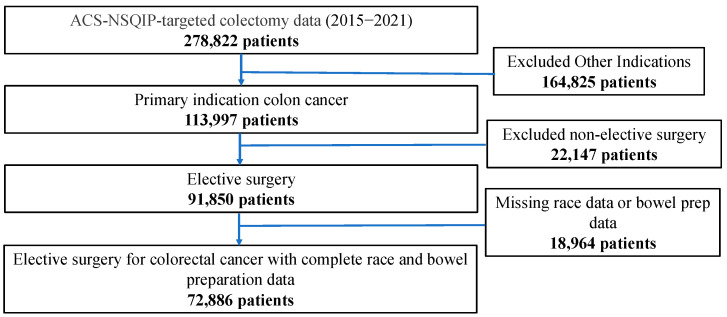
This retrospective cohort study used 2015-2021 ACS-NSQIP-targeted data for elective colectomy for colon cancer. Multivariate regression evaluated predictors of post-operative outcomes: post-operative ileus, anastomotic leak, surgical site infection (SSI), operative time, and hospital length of stay (LOS).
72,886 patients were evaluated with 82.1% White, 11.1% Black, and 6.8% Asian or Asian Pacific Islander (AAPI); 4.2% were Hispanic and 51.4% male. Regression accounting for age, sex, ASA classification, comorbidities, and operative approach showed Black, AAPI, and Hispanic patients were more likely to have had no bowel preparation compared to White patients receiving MBP+OAB. Compared to White patients, Black and AAPI patients had higher odds of prolonged LOS and pro-longed operative time. Black patients had higher odds of post-operative ileus.
Racial disparities exist in both bowel preparation administration and post-operative complications despite the method of bowel preparation. This warrants exploration into discriminatory bowel preparation practices and potential differences in the efficacy of bowel preparation in specific populations due to biological or social differences, which may affect outcomes. Our study is limited by its use of a large database that lacks socioeconomic variables and patient data beyond 30 days.
术前联合使用口服抗生素(OAB)和机械性肠道准备(MBP)是目前择期结直肠手术的推荐方法。很少有人研究肠道准备及随后的术后并发症中的种族差异。
这项回顾性队列研究使用了2015 - 2021年美国外科医师学会国家外科质量改进计划(ACS - NSQIP)针对结肠癌择期结肠切除术的目标数据。多变量回归评估术后结局的预测因素:术后肠梗阻、吻合口漏、手术部位感染(SSI)、手术时间和住院时间(LOS)。
共评估了72,886例患者,其中82.1%为白人,11.1%为黑人,6.8%为亚裔或亚太岛民(AAPI);4.2%为西班牙裔,51.4%为男性。在考虑年龄、性别、美国麻醉医师协会(ASA)分级、合并症和手术方式的回归分析中,与接受MBP + OAB的白人患者相比,黑人、AAPI和西班牙裔患者更有可能未进行肠道准备。与白人患者相比,黑人和AAPI患者住院时间延长和手术时间延长的几率更高。黑人患者术后肠梗阻的几率更高。
无论采用何种肠道准备方法,在肠道准备实施和术后并发症方面都存在种族差异。这值得探讨是否存在歧视性的肠道准备做法,以及由于生物学或社会差异导致特定人群肠道准备效果的潜在差异,这可能会影响结局。我们的研究存在局限性,因为使用的大型数据库缺乏社会经济变量以及超过30天的患者数据。