Valcher Stefano, Villaschi Alessandro, Falasconi Giulio, Chiarito Mauro, Giunti Filippo, Novelli Laura, Addeo Lucio, Taormina Antonio, Panico Cristina, Francia Pietro, Saglietto Andrea, Del Monaco Guido, Latini Alessia Chiara, Carli Sebastiano, Frittella Stefano, Giaj Levra Alessandro, Antonelli Giulia, Preda Alberto, Guarracini Fabrizio, Mazzone Patrizio, Berruezo Antonio, Tritto Massimo, Condorelli Gianluigi, Penela Diego
Department of Biomedical Sciences, Humanitas University, 20072 Pieve Emanuele, Italy.
Olv Hospital, 9300 Aalst, Belgium.
J Clin Med. 2024 Aug 3;13(15):4541. doi: 10.3390/jcm13154541.
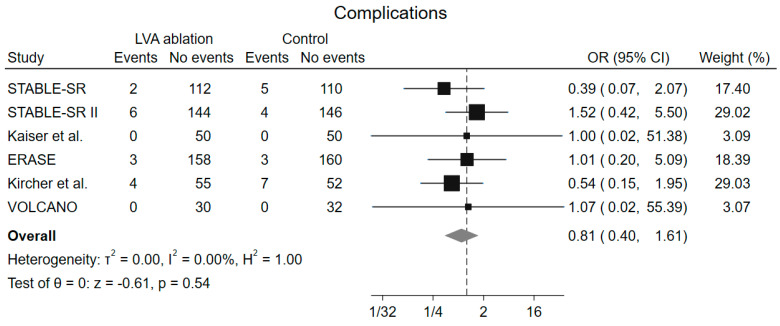
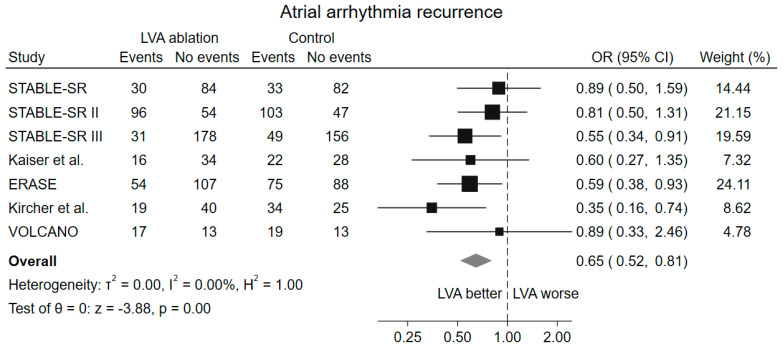
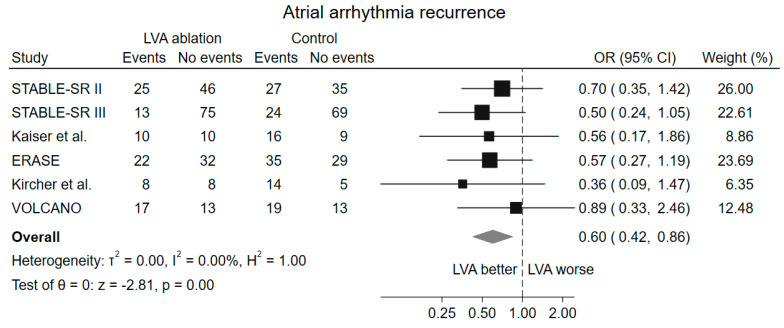
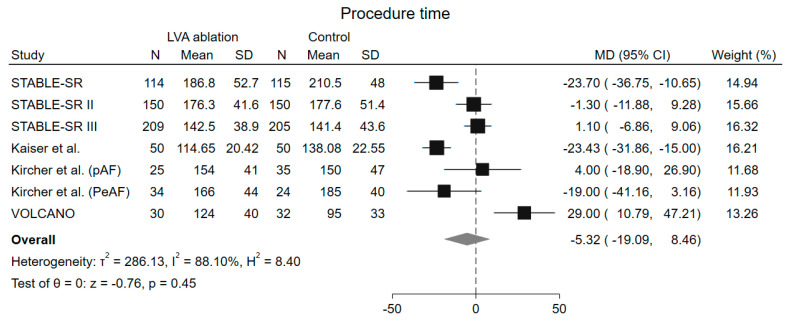
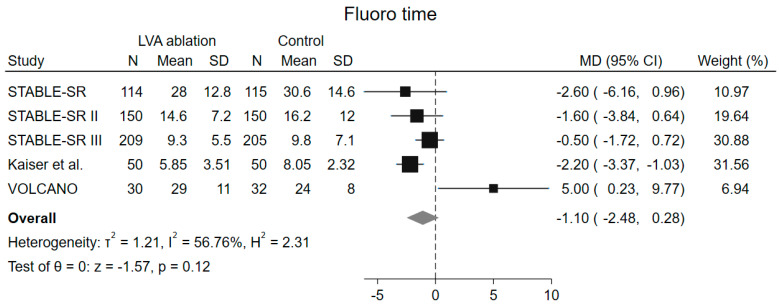
Low-voltage area (LVA) ablation, in addition to pulmonary vein isolation (PVI), has been proposed as a new strategy in patients with atrial fibrillation (AF), but clinical trials have shown conflicting results. We performed a systematic review and meta-analysis to assess the impact of LVA ablation in patient undergoing AF ablation (PROSPERO-registered CRD42024537696). Randomized clinical trials investigating the role of LVA ablation in addition to PVI in patients with AF were searched on PubMed, Embase, and the Cochrane Library from inception to 22 April 2024. Primary outcome was atrial arrhythmia recurrence after the first AF ablation procedure. Secondary endpoints included procedure time, fluoroscopy time, and procedure-related complication rate. Sensitivity analysis including only patients with LVA demonstration at mapping and multiple subgroups analyses were also performed. 1547 patients from 7 studies were included. LVA ablation in addition to PVI reduced atrial arrhythmia recurrence (odds ratio [OR] 0.65, 95% confidence interval [CI] 0.52-0.81, < 0.001) with a number needed to treat to prevent recurrence of 10. No difference in procedure time (mean difference [MD] -5.32 min, 95% CI -19.01-8.46 min, = 0.45), fluoroscopy time (MD -1.10 min, 95% CI -2.48-0.28 min, = 0.12) and complication rate (OR 0.81, 95% CI 0.40-1.61, = 0.54) was observed. Consistent results were demonstrated when considering only patients with LVA during mapping and in prespecified subgroups for AF type (paroxysmal vs. persistent), multicentric vs. monocentric trial, and ablation strategy in control group. : In patients with AF, ablation of LVAs in addition to PVI reduces atrial arrhythmia recurrence without a significant increase in procedure time, fluoroscopy time, or complication rate.
除肺静脉隔离(PVI)外,低电压区(LVA)消融已被提出作为心房颤动(AF)患者的一种新策略,但临床试验结果相互矛盾。我们进行了一项系统评价和荟萃分析,以评估LVA消融对接受AF消融患者的影响(PROSPERO注册编号CRD42024537696)。从创刊至2024年4月22日,在PubMed、Embase和Cochrane图书馆中检索了研究LVA消融联合PVI在AF患者中作用的随机临床试验。主要结局是首次AF消融术后房性心律失常复发。次要终点包括手术时间、透视时间和手术相关并发症发生率。还进行了仅纳入标测时有LVA证据患者的敏感性分析以及多个亚组分析。纳入了来自7项研究的1547例患者。LVA消融联合PVI可降低房性心律失常复发率(优势比[OR]0.65,95%置信区间[CI]0.52 - 0.81,P<0.001),预防复发所需治疗人数为10。手术时间(平均差[MD] - 5.32分钟,95%CI - 19.01 - 8.46分钟,P = 0.45)、透视时间(MD - 1.10分钟,95%CI - 2.48 - 0.28分钟,P = 0.12)和并发症发生率(OR 0.81,95%CI 0.40 - 1.61,P = 0.54)无差异。在仅考虑标测时有LVA的患者以及针对AF类型(阵发性与持续性)、多中心与单中心试验以及对照组消融策略的预先指定亚组中,结果一致。结论:在AF患者中,LVA消融联合PVI可降低房性心律失常复发率,且手术时间、透视时间或并发症发生率无显著增加。