Department of Allergy and Clinical Immunology, State Key Laboratory of Respiratory Disease, National Center for Respiratory Medicine, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital, Guangzhou Medical University, Guangzhou, People's Republic of China.
Johns Hopkins Asthma & Allergy Center, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Respir Res. 2024 Aug 10;25(1):304. doi: 10.1186/s12931-024-02943-7.
The gut-lung axis, pivotal for respiratory health, is inadequately explored in pulmonary and critical care medicine (PCCM) inpatients.
Examining PCCM inpatients from three medical university-affiliated hospitals, we conducted 16S ribosomal RNA sequencing on stool samples (inpatients, n = 374; healthy controls, n = 105). We conducted statistical analyses to examine the gut microbiota composition in PCCM inpatients, comparing it to that of healthy controls. Additionally, we explored the associations between gut microbiota composition and various clinical factors, including age, white blood cell count, neutrophil count, platelet count, albumin level, hemoglobin level, length of hospital stay, and medical costs.
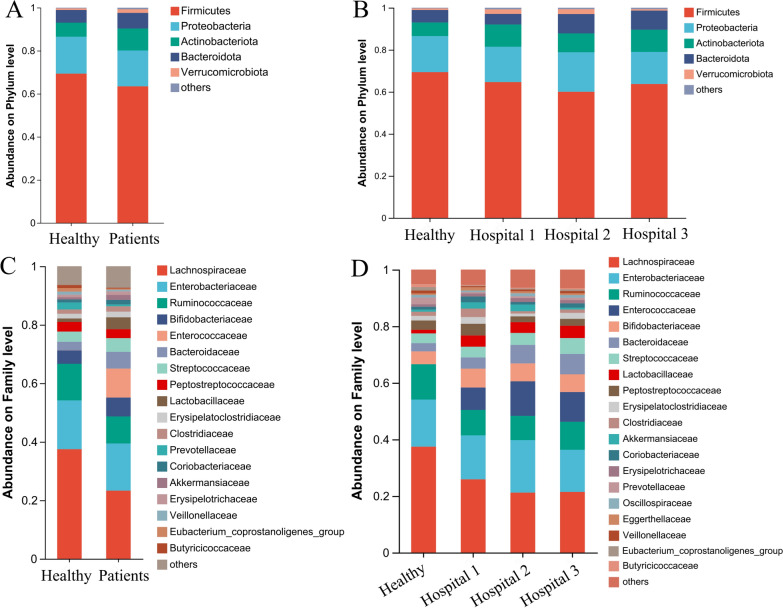
PCCM inpatients exhibited lower gut microbiota diversity than healthy controls. Principal Coordinates Analysis revealed marked overall microbiota structure differences. Four enterotypes, including the exclusive Enterococcaceae enterotype in inpatients, were identified. Although no distinctions were found at the phylum level, 15 bacterial families exhibited varying abundances. Specifically, the inpatient population from PCCM showed a significantly higher abundance of Enterococcaceae, Lactobacillaceae, Erysipelatoclostridiaceae, Clostridiaceae, and Tannerellaceae. Using random forest analyses, we calculated the areas under the receiver operating characteristic curves (AUCs) to be 0.75 (95% CIs 0.69-0.80) for distinguishing healthy individuals from inpatients. The four most abundant genera retained in the classifier were Blautia, Subdoligranulum, Enterococcus, and Klebsiella.
Evidence of gut microbiota dysbiosis in PCCM inpatients underscores the gut-lung axis's significance, promising further avenues in respiratory health research.
肠道-肺部轴对于呼吸健康至关重要,但在肺科和危重病医学(PCCM)住院患者中尚未得到充分探索。
我们对来自三所医科大学附属医院的 PCCM 住院患者进行了粪便样本 16S 核糖体 RNA 测序(住院患者 n=374;健康对照 n=105)。我们进行了统计分析,以比较 PCCM 住院患者和健康对照者的肠道微生物群落组成。此外,我们还探讨了肠道微生物群落组成与各种临床因素(包括年龄、白细胞计数、中性粒细胞计数、血小板计数、白蛋白水平、血红蛋白水平、住院时间和医疗费用)之间的关联。
PCCM 住院患者的肠道微生物群落多样性低于健康对照者。主坐标分析显示整体微生物群落结构存在明显差异。确定了四种肠型,包括住院患者特有的肠球菌肠型。虽然在门水平上没有发现差异,但有 15 个细菌家族的丰度存在差异。具体而言,PCCM 住院患者人群中肠球菌科、乳杆菌科、丹毒丝菌科、梭菌科和 Tannerellaceae 的丰度显著较高。使用随机森林分析,我们计算出区分健康个体和住院患者的接收者操作特征曲线下面积(AUC)为 0.75(95%CI 0.69-0.80)。保留在分类器中的四个最丰富的属是布劳特氏菌属、副拟杆菌属、肠球菌属和克雷伯菌属。
PCCM 住院患者肠道微生物群落失调的证据强调了肠道-肺部轴的重要性,为呼吸健康研究开辟了新的途径。