Kereiakes Dean J, Hill Jonathan M, Shlofmitz Richard A, Klein Andrew J, Riley Robert F, Price Matthew J, Herrmann Howard C, Bachinsky William, Waksman Ron, Stone Gregg W
The Christ Hospital and Lindner Research Center, Cincinnati, OH, USA.
Royal Brompton Hospital, London, United Kingdom.
J Soc Cardiovasc Angiogr Interv. 2022 Jan 30;1(1):100001. doi: 10.1016/j.jscai.2021.100001. eCollection 2022 Jan-Feb.
Coronary calcification impairs stent delivery and optimal expansion, a significant predictor of subsequent stent thrombosis and restenosis. Current calcium ablative technologies may be limited by guidewire bias and periprocedural complications. Intravascular lithotripsy (IVL) delivers acoustic pressure waves to modify calcium, enhance vessel compliance, and optimize stent deployment. The Disrupt CAD III study demonstrated high (92.4%) procedural success and low (7.8%) 30-day major adverse cardiac event (MACE) rates following IVL, but longer term follow-up is required to determine the durability of clinical benefit and the late impact of optimized stent implantation associated with IVL. This analysis evaluates 1-year outcomes from the Disrupt CAD III study.
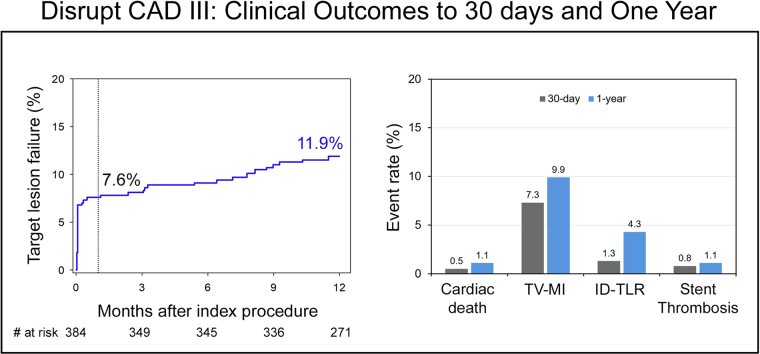
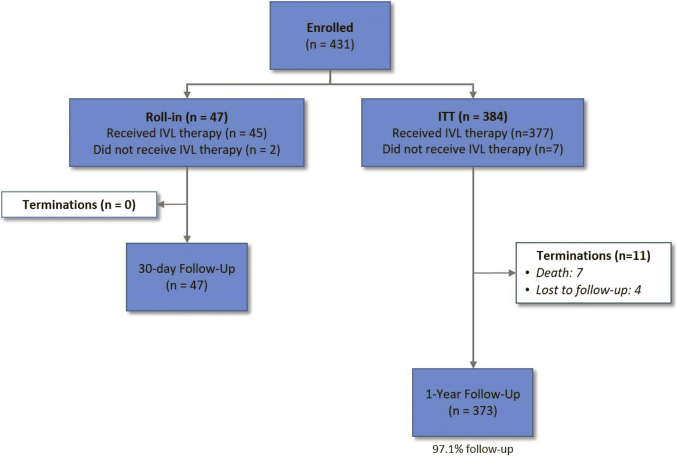
Disrupt CAD III (NCT03595176) was a prospective, single-arm approval study designed to assess the safety and effectiveness of IVL as an adjunct to coronary stenting in , severely calcified coronary lesions ( = 384). MACE was defined as the composite of cardiac death, myocardial infarction (MI), or ischemia-driven target vessel revascularization; target lesion failure was defined as cardiac death, MI, or ischemia-driven target lesion revascularization (ID-TLR).
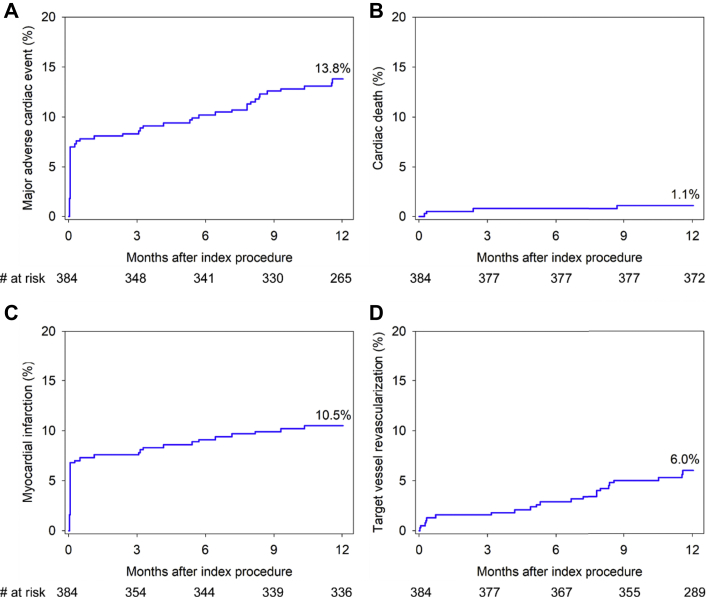
At 1 year, MACE occurred in 13.8% of patients (cardiac death: 1.1%, MI: 10.5%, ischemia-driven target vessel revascularization: 6.0%) and target lesion failure occurred in 11.9% (ID-TLR: 4.3%), both driven by non-Q-wave MI (9.2%). Stent thrombosis (definite or probable) occurred in 1.1% of patients (including 1 event [0.3%] beyond 30 days).
Disrupt CAD III represents the largest long-term (1-year) analysis of coronary IVL to date. IVL treatment prior to coronary stent implantation in severely calcified lesions was associated with low 1-year rates of MACE, ID-TLR, and stent thrombosis.
冠状动脉钙化会影响支架输送及最佳扩张效果,是后续支架血栓形成和再狭窄的重要预测指标。当前的消钙技术可能受导丝偏差和围手术期并发症的限制。血管内碎石术(IVL)可传递声压波来改变钙成分、增强血管顺应性并优化支架植入。Disrupt CAD III研究显示,IVL术后的手术成功率较高(92.4%),30天主要不良心脏事件(MACE)发生率较低(7.8%),但需要更长时间的随访来确定临床获益的持久性以及与IVL相关的优化支架植入的后期影响。本分析评估了Disrupt CAD III研究的1年结局。
Disrupt CAD III(NCT03595176)是一项前瞻性单臂批准研究,旨在评估IVL作为严重钙化冠状动脉病变(n = 384)冠状动脉支架置入术辅助手段的安全性和有效性。MACE定义为心源性死亡、心肌梗死(MI)或缺血驱动的靶血管血运重建的复合事件;靶病变失败定义为心源性死亡、MI或缺血驱动的靶病变血运重建(ID-TLR)。
1年时,13.8%的患者发生MACE(心源性死亡:1.1%,MI:10.5%,缺血驱动的靶血管血运重建:6.0%),11.9%的患者发生靶病变失败(ID-TLR:4.3%),两者均由非Q波MI(9.2%)导致。1.1%的患者发生支架血栓形成(确诊或可能)(包括1例30天以上的事件[0.3%])。
Disrupt CAD III是迄今为止对冠状动脉IVL最大规模的长期(1年)分析。在严重钙化病变中,冠状动脉支架植入术前进行IVL治疗与1年时较低的MACE、ID-TLR和支架血栓形成发生率相关。