Koseki Akihito, Suzuki Youji, Uchida Shugo, Morishita Naoki, Hokazono Yukio, Kuriki Ken, Yamamura Yasuhiro, Yoshida Mari, Sakai Naoki
Neurology, Yaizu City Hospital, Yaizu, JPN.
Diagnostic Pathology, Yaizu City Hospital, Yaizu, JPN.
Cureus. 2024 Jul 11;16(7):e64358. doi: 10.7759/cureus.64358. eCollection 2024 Jul.
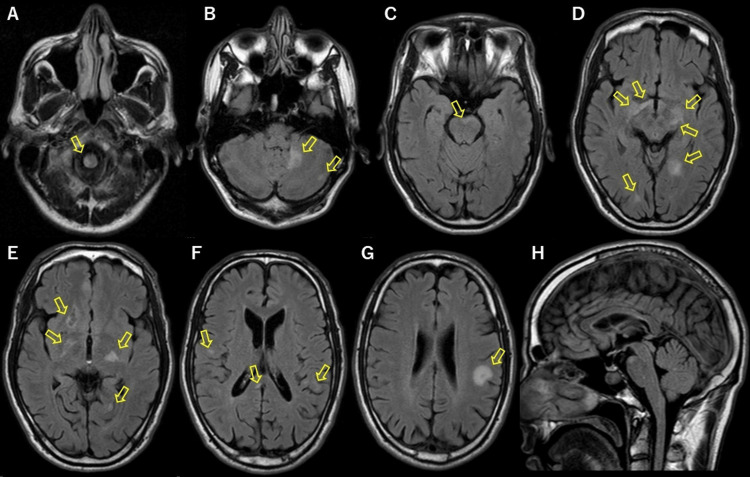
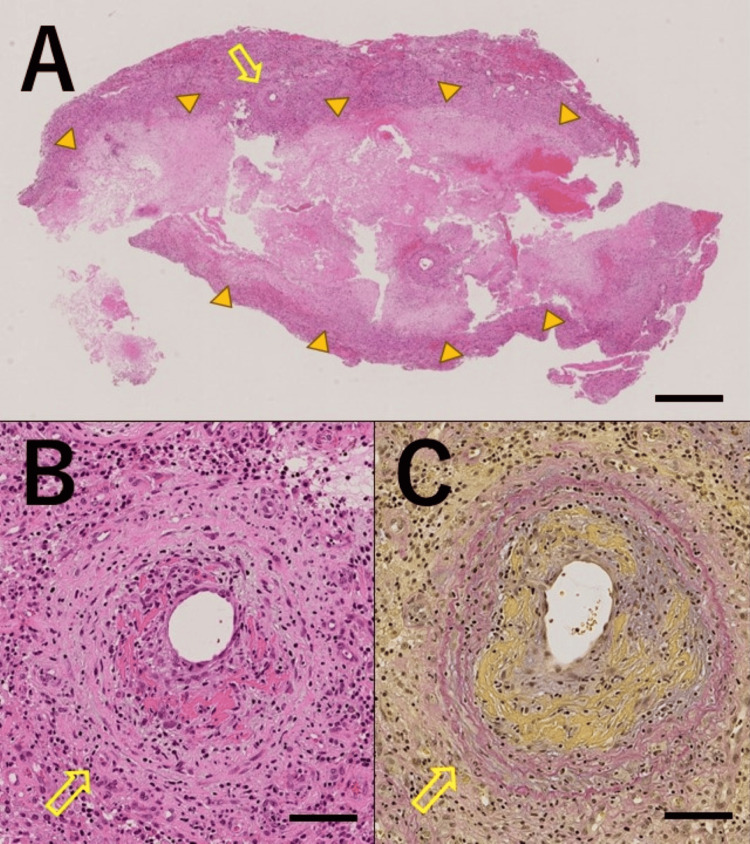
Primary central nervous system vasculitis (PCNSV) is an angiitis localized to the central nervous system (CNS), with various manifestations and no specific biomarkers. Herein, we report a case of PCNSV that presented with an unusual course. A 40-year-old Japanese male developed inner ear symptoms and visual field disturbances. Later, at 42 years of age, the patient developed right hemiparesis and was diagnosed with multiple sclerosis (MS). He received methylprednisolone pulse therapy, which improved his symptoms and resolved most brain lesions. Subsequently, he did not visit the hospital for 13 years, during which time he experienced no relapse. At 55 years of age, he presented to our hospital with fatigue and dizziness. Susac syndrome was suspected because of sensorineural hearing loss and snowball lesions in the corpus callosum. Some of the brain lesions resolved spontaneously. A biopsy was performed on a right frontal lobe lesion, which revealed vasculitis with fibrinoid necrosis, no demyelinating lesions, no amyloid positivity, and no infiltration of atypical lymphocytes. With no evidence of vasculitis in other organs, the patient was diagnosed with PCNSV. The patient was treated with methylprednisolone pulse therapy, followed by oral prednisolone (1 mg/kg/day). The prednisolone was tapered off, and no relapse of symptoms or new lesions on magnetic resonance imaging (MRI) were noted. As observed in this case, even in a scenario suggestive of Susac syndrome or multiple sclerosis, PCNSV should be considered a differential diagnosis and confirmed via brain biopsy.
原发性中枢神经系统血管炎(PCNSV)是一种局限于中枢神经系统(CNS)的血管炎,有多种表现且无特异性生物标志物。在此,我们报告一例病程异常的PCNSV病例。一名40岁的日本男性出现内耳症状和视野障碍。后来,在42岁时,该患者出现右侧偏瘫,被诊断为多发性硬化症(MS)。他接受了甲泼尼龙冲击治疗,症状得到改善,大多数脑病变消失。随后,他有13年未就医,在此期间未复发。55岁时,他因疲劳和头晕前来我院就诊。由于感音神经性听力损失和胼胝体出现“雪球样”病变,怀疑为Susac综合征。部分脑病变自行消失。对右侧额叶病变进行活检,结果显示为伴有纤维蛋白样坏死的血管炎,无脱髓鞘病变,无淀粉样蛋白阳性,无非典型淋巴细胞浸润。由于其他器官无血管炎证据,该患者被诊断为PCNSV。患者接受了甲泼尼龙冲击治疗,随后口服泼尼松龙(1 mg/kg/天)。泼尼松龙逐渐减量,未观察到症状复发或磁共振成像(MRI)出现新病变。正如本病例所示,即使在疑似Susac综合征或多发性硬化症的情况下,PCNSV也应被视为鉴别诊断,并通过脑活检进行确诊。