Stefanescu Schmidt Ada C, Armstrong Aimee, Kennedy Kevin F, Inglessis-Azuaje Ignacio, Horlick Eric M, Holzer Ralf J, Bhatt Ami B
Division of Cardiology, Massachusetts General Hospital, Boston, Massachusetts.
The Heart Center, Nationwide Children's Hospital, Columbus, Ohio.
J Soc Cardiovasc Angiogr Interv. 2022 Jul 1;1(5):100393. doi: 10.1016/j.jscai.2022.100393. eCollection 2022 Sep-Oct.
Although surgical repair was the traditional first-line treatment for native coarctation of the aorta (CoA), balloon angioplasty (BA) and stenting are now increasingly being performed. We aimed to determine the practice patterns and acute outcomes of transcatheter interventions for native coarctation in the largest multicenter registry for congenital catheterization.
CoA interventions from the IMPACT (IMproving Pediatric and Adult Congenital Treatment) National Cardiovascular Data Registry were analyzed. The procedure choice and acute outcomes were compared among patients with no prior interventions on the aortic isthmus (native CoA). Procedural success was defined as no major adverse events (MAEs) and a final peak gradient of <20 mm Hg and optimal outcome as no MAEs and a final gradient of <10 mm Hg.
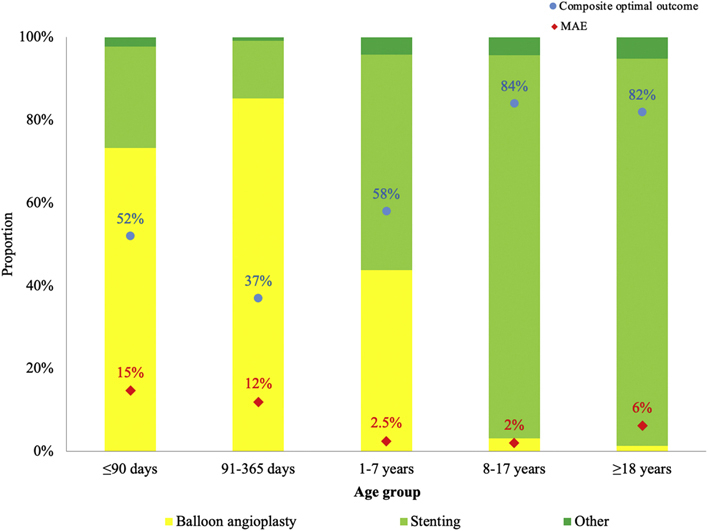
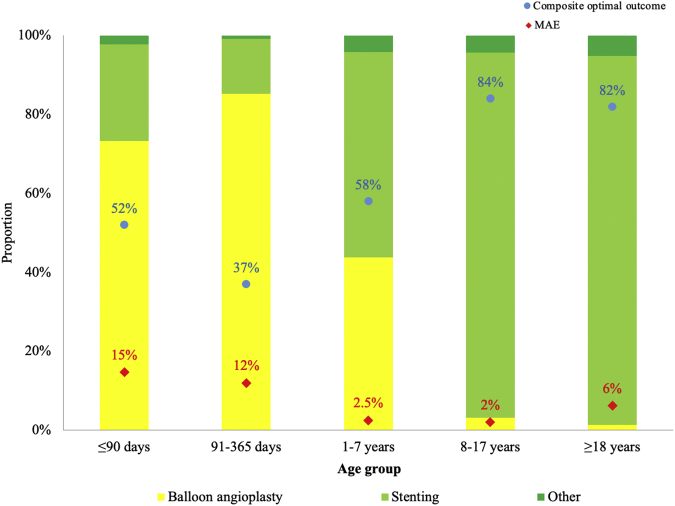
Over the 8-year study period, 5928 CoA procedures were performed, of which 1187 were performed in patients with native CoA. In this group, stenting was performed in more then half of children aged >1 year and >90% of those aged >8 years. Procedural success was achieved in >90% of stenting procedures but in only 69% of BAs. Stent implantation was associated with a higher likelihood of optimal gradient (<10 mm Hg) after adjustment for age and baseline characteristics. MAEs were most common in children aged <1 year (14%), occurred in 2% to 2.5% of those aged 1 to 18 years and in 6.6% of adults ( < .001), and were more likely after BA than after stenting (odds ratio, 0.5; 95% CI, 0.28-0.9; unadjusted = .02).
Catheter interventions for native coarctation are performed safely in older children and adults, with a high degree of immediate procedural success, particularly with stenting.
尽管手术修复曾是主动脉缩窄(CoA)传统的一线治疗方法,但如今球囊血管成形术(BA)和支架置入术的应用越来越广泛。我们旨在通过最大的先天性导管插入术多中心登记处,确定经导管介入治疗原发性主动脉缩窄的实践模式和急性结果。
对来自IMPACT(改善儿童和成人先天性治疗)国家心血管数据登记处的CoA介入治疗进行分析。比较主动脉峡部未接受过先前干预的患者(原发性CoA)的手术选择和急性结果。手术成功定义为无重大不良事件(MAE)且最终峰值梯度<20 mmHg,最佳结果定义为无MAE且最终梯度<10 mmHg。
在8年的研究期间,共进行了5928例CoA手术,其中1187例是针对原发性CoA患者。在该组中,超过一半的1岁以上儿童和超过90%的8岁以上儿童接受了支架置入术。超过90%的支架置入手术取得了成功,但BA手术的成功率仅为69%。在调整年龄和基线特征后,支架植入与获得最佳梯度(<10 mmHg)的可能性更高相关。MAE在1岁以下儿童中最为常见(14%),在1至18岁儿童中发生率为2%至2.5%,在成人中为6.6%(P<0.001),且BA术后发生MAE的可能性高于支架置入术后(优势比,0.5;95%CI,0.28 - 0.9;未调整P = 0.02)。
对大龄儿童和成人进行原发性主动脉缩窄的导管介入治疗是安全的,手术即刻成功率高,尤其是支架置入术。