Rymer Jennifer, Alhanti Brooke, Kemp Steven, Bhatt Deepak L, Kochar Ajar, Angiolillo Dominick J, Diaz Miguel, Garratt Kirk N, Wimmer Neil J, Waksman Ron, Kirtane Ajay J, Ang Lawrence, Bach Richard, Barker Colin, Jenkins Ronald, Basir Mir B, Sullivan Alex, El-Sabae Hijrah, Brothers Leo, Ohman E Magnus, Jones W Schuyler, Washam Jeffrey B, Wang Tracy Y
Division of Cardiology, Duke University School of Medicine, Durham, North Carolina.
Duke Clinical Research Institute, Durham, North Carolina.
J Soc Cardiovasc Angiogr Interv. 2023 Nov 27;3(2):101202. doi: 10.1016/j.jscai.2023.101202. eCollection 2024 Feb.
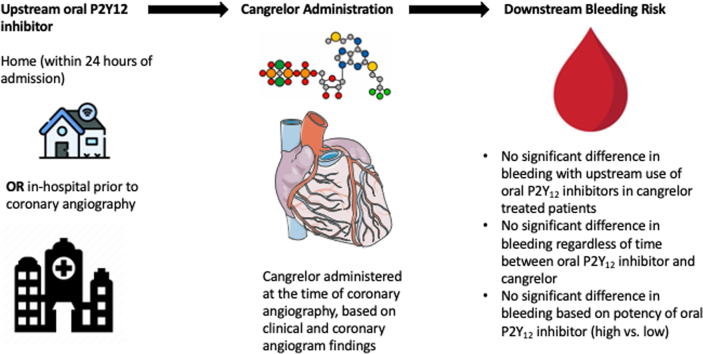
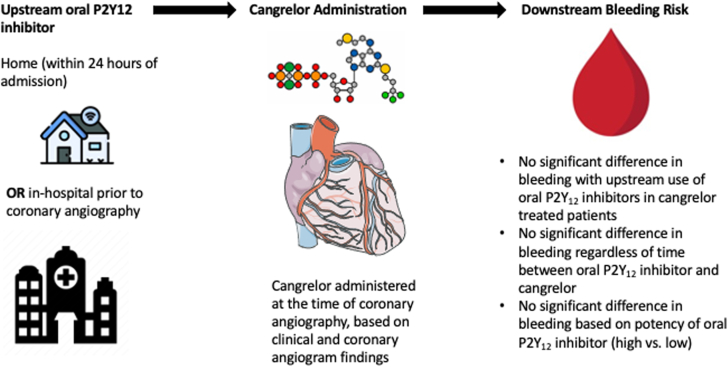
Little is known about the bleeding risk associated with cangrelor use in patients with myocardial infarction (MI) who are exposed to an oral P2Y inhibitor before coronary angiography.
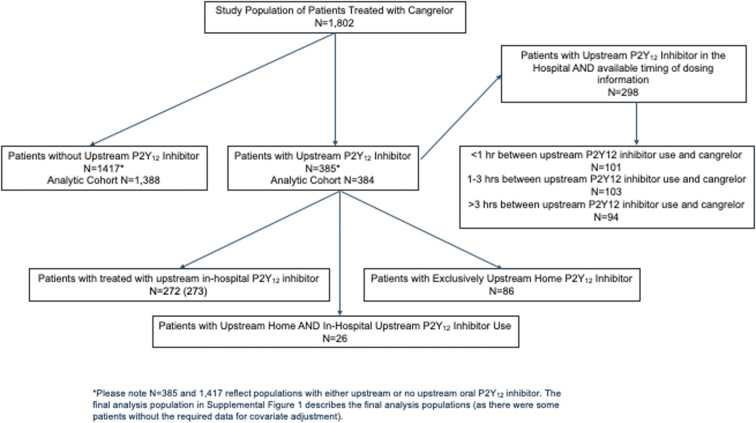
Cangrelor in Acute MI: Effectiveness and Outcomes (CAMEO) is an observational registry studying platelet inhibition for patients with MI. Upstream oral P2Y inhibition was defined as receipt of an oral P2Y inhibitor within 24 hours before hospitalization or in-hospital before angiography. Among cangrelor-treated patients, we compared bleeding after cangrelor use through 7 days postdischarge between patients with and without upstream oral P2Y inhibitor exposure.
Among 1802 cangrelor-treated patients with MI, 385 (21.4%) received upstream oral P2Y inhibitor treatment. Of these, 101 patients (33.8%) started cangrelor within 1 hour, 103 (34.4%) between 1 and 3 hours, and 95 (31.8%), >3 hours after in-hospital oral P2Y inhibitor administration; the remaining received an oral P2Y inhibitor before hospitalization. There was no statistically significant difference in rates of bleeding among cangrelor-treated patients with and without upstream oral P2Y inhibitor exposure (6.5% vs 8.8%; adjusted odds ratio [OR], 0.62; 95% CI, 0.38-1.01). Bleeding was observed in 5.0%, 10.7%, and 3.2% of patients treated with cangrelor <1, 1 to 3, and >3 hours after the last oral PY inhibitor dose, respectively; bleeding rates were not statistically different between groups (1-3 hours vs <1 hour: adjusted OR, 2.70; 95% CI, 0.87-8.32; >3 hours vs <1 hour: adjusted OR, 0.65; 95% CI, 0.15-2.85).
Bleeding risk was not observed to be significantly higher after cangrelor treatment in patients with and without upstream oral P2Y12 inhibitor exposure.
对于在冠状动脉造影前使用过口服P2Y抑制剂的心肌梗死(MI)患者,使用坎格雷洛的出血风险知之甚少。
坎格雷洛在急性心肌梗死中的应用:有效性和结局(CAMEO)是一项观察性登记研究,旨在研究MI患者的血小板抑制情况。上游口服P2Y抑制定义为在住院前24小时内或住院期间血管造影前接受口服P2Y抑制剂治疗。在接受坎格雷洛治疗的患者中,我们比较了有或没有上游口服P2Y抑制剂暴露的患者在使用坎格雷洛后至出院后7天内的出血情况。
在1802例接受坎格雷洛治疗的MI患者中,385例(21.4%)接受了上游口服P2Y抑制剂治疗。其中,101例患者(33.8%)在1小时内开始使用坎格雷洛,103例(34.4%)在1至3小时内开始使用,95例(31.8%)在住院口服P2Y抑制剂给药后3小时以上开始使用;其余患者在住院前接受了口服P2Y抑制剂治疗。有或没有上游口服P2Y抑制剂暴露的坎格雷洛治疗患者的出血率无统计学显著差异(6.5%对8.8%;调整后的优势比[OR],0.62;95%置信区间,0.38 - 1.01)。在最后一剂口服P2Y抑制剂后<1小时、1至3小时和>3小时接受坎格雷洛治疗的患者中,出血发生率分别为5.0%、10.7%和3.2%;各组之间的出血率无统计学差异(1至3小时对<1小时:调整后的OR,2.70;95%置信区间,0.87 - 8.32;>3小时对<1小时:调整后的OR,0.65;95%置信区间,0.15 - 2.85)。
在有或没有上游口服P2Y12抑制剂暴露的患者中,坎格雷洛治疗后未观察到出血风险显著升高。