Langreen S, Ludwikowski B, Dingemann J, Ure B M, Hofmann A D, Kuebler J F
Pediatric Surgery Clinic, Center for Pediatrics and Adolescent Medicine, Hannover Medical School, Hanover, Germany.
Department of Pediatric Surgery, Kinder- und Jugendkrankenhaus AUF DER BULT, Hanover, Germany.
Front Pediatr. 2024 Jul 26;12:1397614. doi: 10.3389/fped.2024.1397614. eCollection 2024.
Dismembered laparoscopic pyeloplasty (LP) is a well-accepted treatment modality for ureteropelvic junction obstruction (UPJO) in children. However, its efficacy and safety in infants, particularly neonates, remain uncertain. To address this significant knowledge gap, we aimed to compare outcomes between a cohort of neonates and infants undergoing LP vs. open pyeloplasty (OP) at less than 6 months and 6 weeks of age.
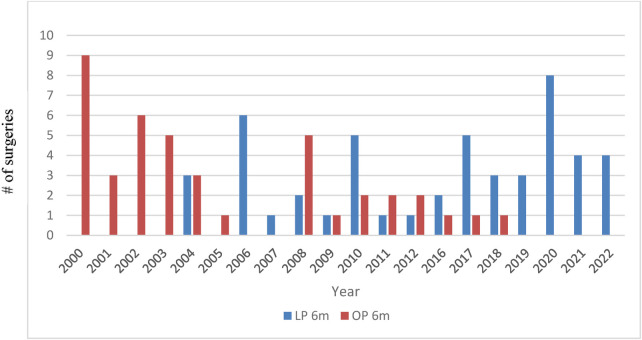
We conducted a retrospective analysis of data from patients who underwent primary pyeloplasty at our institution between 2000 and 2022. Only patients aged 6 months or less at the time of surgery were included, excluding redo-procedures or conversions. Ethical approval was obtained, and data were assessed for redo-pyeloplasty and postoperative complications, classified according to the Clavien-Madadi classification. A standard postoperative assessment was performed 6 weeks postoperatively. This included an isotope scan and a routine ultrasound up to the year 2020.
A total of 91 eligible patients were identified, of which 49 underwent LP and 42 underwent OP. Patients receiving LP had a median age of 11.4 (1-25.4) weeks, compared to 13.8 (0.5-25.9) weeks for those receiving OP ( > 0.31). Both groups in our main cohort had an age range of 0-6 months at the time of surgery. Nineteen patients were younger than 6 weeks at the time of surgery. The mean operating time was longer for LP (161 ± 43 min) than that for OP (109 ± 32 min, < 0.001). However, the mean operating time was not longer in the patient group receiving LP at ≤6 weeks (145 ± 21.6) compared to that in our main cohort receiving LP. There was no significant difference in the length of stay between the groups. Four patients after LP required emergency nephrostomy compared to one patient after OP. The rate of revision pyeloplasty in our main cohort aged 0-6 months at surgery was 8% in the patient group receiving LP and 14% in the patient group receiving OP (not significant). Three revisions after LP were due to persistent UPJO, and one was due to stent migration. Only one patient requiring revision pyeloplasty was less than 6 weeks old.
To our knowledge, this is one of the largest collectives of laparoscopic pyeloplasty performed in infants, and it is the youngest cohort published to date. Based on our experience, LP in neonates and infants under 6 months appears to be as effective as open surgery.
腹腔镜离断式肾盂成形术(LP)是治疗儿童输尿管肾盂连接部梗阻(UPJO)的一种广泛接受的治疗方式。然而,其在婴儿尤其是新生儿中的疗效和安全性仍不确定。为了填补这一重大知识空白,我们旨在比较一组年龄小于6个月和6周的接受LP与开放肾盂成形术(OP)的新生儿和婴儿的治疗效果。
我们对2000年至2022年在我院接受初次肾盂成形术的患者数据进行了回顾性分析。仅纳入手术时年龄在6个月及以下的患者,排除再次手术或中转手术。获得伦理批准,并根据Clavien-Madadi分类法评估再次肾盂成形术和术后并发症的数据。术后6周进行标准的术后评估。2020年前这包括同位素扫描和常规超声检查。
共确定91例符合条件的患者,其中49例接受了LP,42例接受了OP。接受LP的患者中位年龄为11.4(1 - 25.4)周,接受OP的患者中位年龄为13.8(0.5 - 25.9)周(P>0.31)。我们主要队列中的两组患者手术时年龄范围均为0 - 六个月。19例患者手术时年龄小于6周。LP的平均手术时间(161±43分钟)比OP的平均手术时间(109±32分钟,P<0.001)长。然而,与我们接受LP的主要队列相比,年龄≤6周接受LP的患者组平均手术时间并不长(1