Vyas Rohit, Changal Khalid H, Bhuta Sapan, Pasadyn Vanessa, Katterle Konrad, Niedoba Matthew J, Vora Keyur, Dharmakumar Rohan, Gupta Rajesh
Division of Cardiovascular Medicine, University of Toledo, Toledo, Ohio.
Department of Internal Medicine, University of Toledo, Toledo, Ohio.
J Soc Cardiovasc Angiogr Interv. 2022 Aug 26;1(6):100444. doi: 10.1016/j.jscai.2022.100444. eCollection 2022 Nov-Dec.
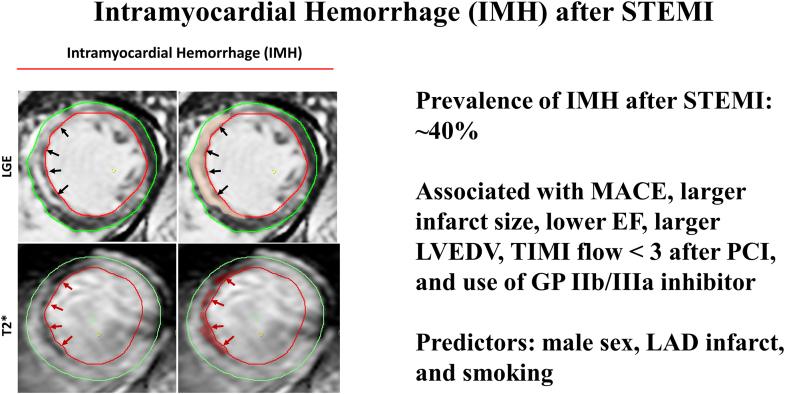
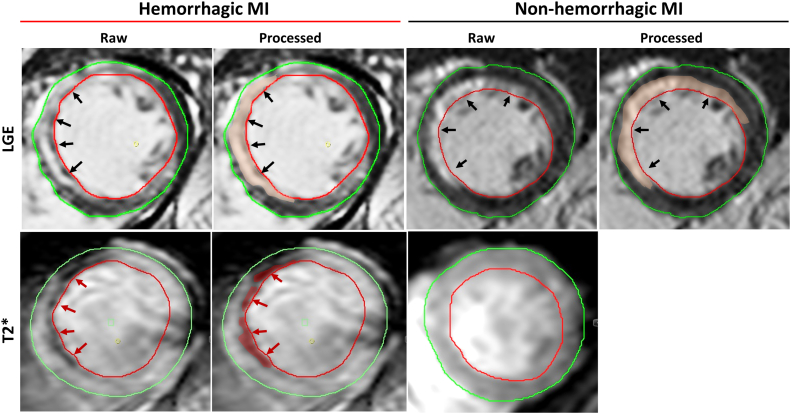
Intramyocardial hemorrhage (IMH) occurs after ST-elevation myocardial infarction (STEMI) and has been documented using cardiac magnetic resonance imaging. The prevalence and prognostic significance of IMH are not well described, and the small sample size has limited prior studies.
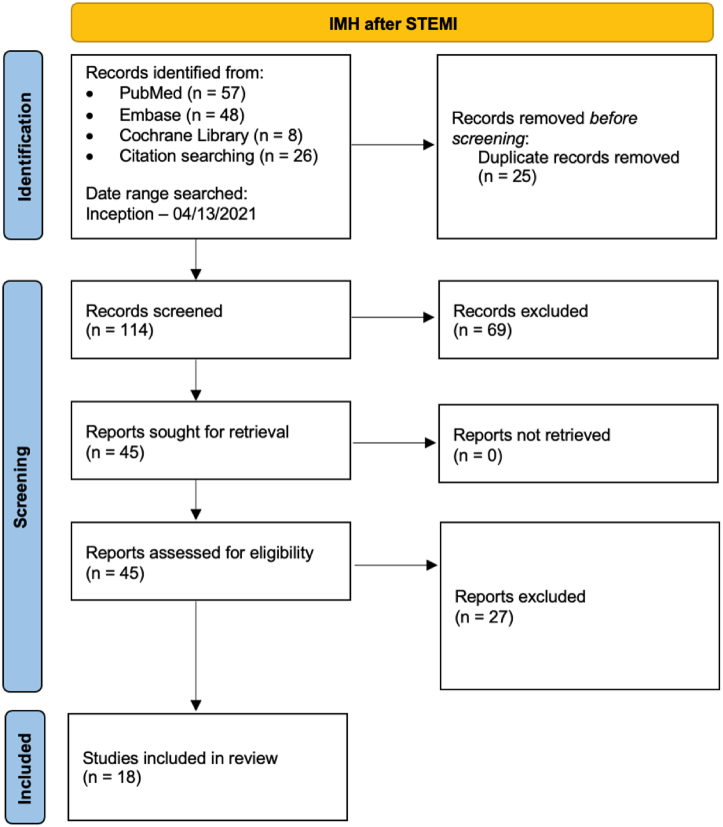
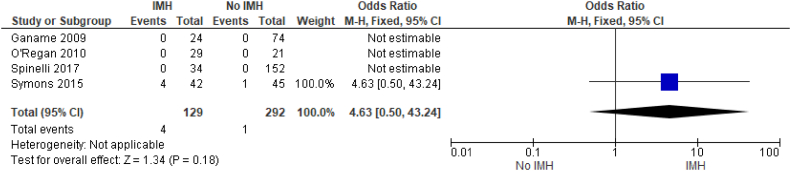
We performed a comprehensive literature search of multiple databases to identify studies that compared outcomes in STEMI patients with or without IMH. The outcomes studied were major adverse cardiovascular events (MACE), infarct size, thrombolysis in myocardial infarction (TIMI) flow after percutaneous coronary intervention (PCI), left ventricular end-diastolic volume (LVEDV), left ventricular ejection fraction (LVEF), and mortality. Odds ratios (ORs) and standardized mean differences with corresponding 95% CIs were calculated using a random effects model.
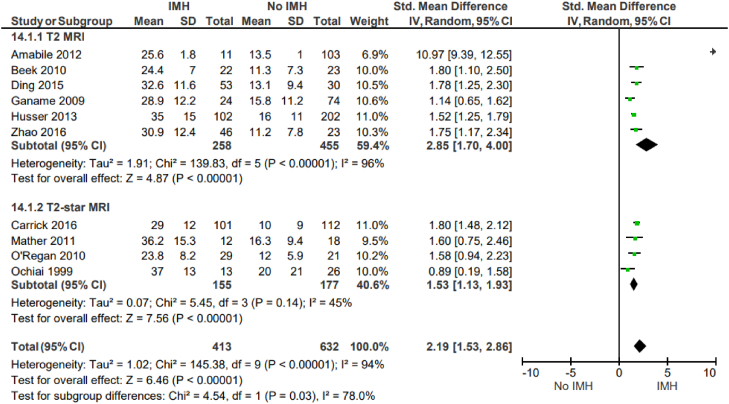
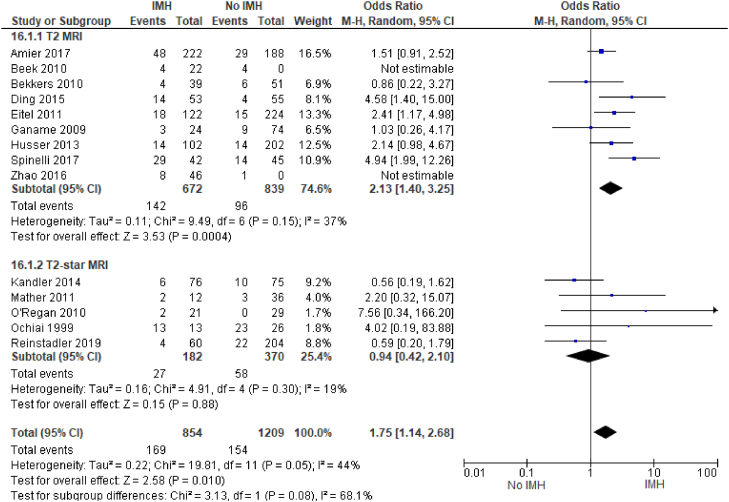
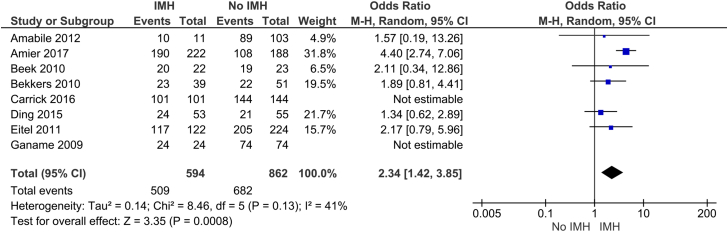
Eighteen studies, including 2824 patients who experienced STEMI (1078 with IMH and 1746 without IMH), were included. The average prevalence of IMH was 39%. There is a significant association between IMH and subsequent MACE (OR, 2.63; 95% CI, 1.79-3.86; < .00001), as well as IMH and TIMI grade <3 after PCI (OR, 1.75; 95% CI, 1.14-2.68; = .05). We also found a significant association between IMH and the use of glycoprotein IIb/IIIa inhibitors (OR, 2.34; 95% CI, 1.42-3.85; = .0008). IMH has a positive association with infarct size (standardized mean difference, 2.19; 95% CI, 1.53-2.86; < .00001) and LVEDV (standardized mean difference, 0.7; 95% CI, 0.41-0.99; < .00001) and a negative association with LVEF (standardized mean difference, -0.89; 95% CI, -1.15 to -0.63; = .01). Predictors of IMH include male sex, smoking, and left anterior descending infarct.
Intramyocardial hemorrhage is prevalent in approximately 40% of patients who experience STEMI. IMH is a significant predictor of MACE and is associated with larger infarct size, higher LVEDV, and lower LVEF after STEMI.
心肌内出血(IMH)发生于ST段抬高型心肌梗死(STEMI)后,已通过心脏磁共振成像得到证实。IMH的患病率及预后意义尚未得到充分描述,且既往研究样本量较小。
我们对多个数据库进行了全面的文献检索,以确定比较有或无IMH的STEMI患者结局的研究。所研究的结局包括主要不良心血管事件(MACE)、梗死面积、经皮冠状动脉介入治疗(PCI)后心肌梗死溶栓(TIMI)血流、左心室舒张末期容积(LVEDV)、左心室射血分数(LVEF)和死亡率。使用随机效应模型计算比值比(OR)和标准化均数差及其相应的95%置信区间。
纳入18项研究,共2824例发生STEMI的患者(1078例有IMH,1746例无IMH)。IMH的平均患病率为39%。IMH与随后的MACE之间存在显著关联(OR = 2.63;95% CI:1.79 - 3.86;P <.00001),以及IMH与PCI后TIMI分级<3之间也存在显著关联(OR = 1.75;95% CI:1.14 - 2.68;P = 0.05)。我们还发现IMH与糖蛋白IIb/IIIa抑制剂的使用之间存在显著关联(OR = 2.34;95% CI:1.42 - 3.85;P = 0.0008)。IMH与梗死面积呈正相关(标准化均数差 = 2.19;95% CI:1.53 - 2.86;P <.00001)和LVEDV呈正相关(标准化均数差 = 0.7;95% CI:0.41 - 0.99;P <.00001),与LVEF呈负相关(标准化均数差 = -0.89;95% CI:-1.15至-0.63;P = 0.01)。IMH的预测因素包括男性、吸烟和左前降支梗死。
心肌内出血在约40%的STEMI患者中普遍存在。IMH是MACE的重要预测因素,并且与STEMI后更大的梗死面积、更高的LVEDV和更低的LVEF相关。