Michaud Erinleigh, Pan Michael, Lakhter Vladimir, Reddy Maligireddy Anand, Hyder Syed N, Patel Nimai, Moles Victor M, McLaughlin Vallerie V, Agarwal Prachi P, Visovatti Scott H, Cascino Thomas M, Haft Jonathan, Rosenfield Kenneth, Nallamothu Brahmajee K, Giri Jay S, Bashir Riyaz, Aggarwal Vikas
Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan.
Division of Cardiology, Department of Medicine, Harbor-UCLA Medical Center, Torrance, California.
J Soc Cardiovasc Angiogr Interv. 2023 Jul 25;2(5):101108. doi: 10.1016/j.jscai.2023.101108. eCollection 2023 Sep-Oct.
Catheter-based interventions have emerged for both acute and chronic pulmonary thromboembolic disease. With this development and the need for segmental cannulation, anatomic understanding of pulmonary arterial segmental branch origination is important. We aim to describe the prevalence of different pulmonary arterial segmental branch origination patterns.
This study included 179 consecutive patients who underwent bilateral nonselective invasive pulmonary angiography for the evaluation of chronic thromboembolic pulmonary hypertension.
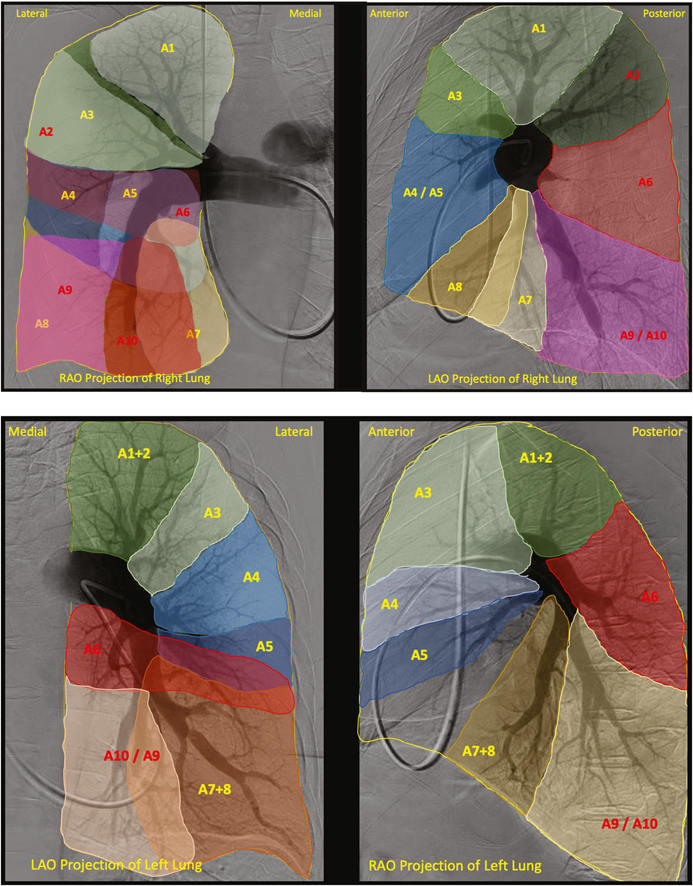
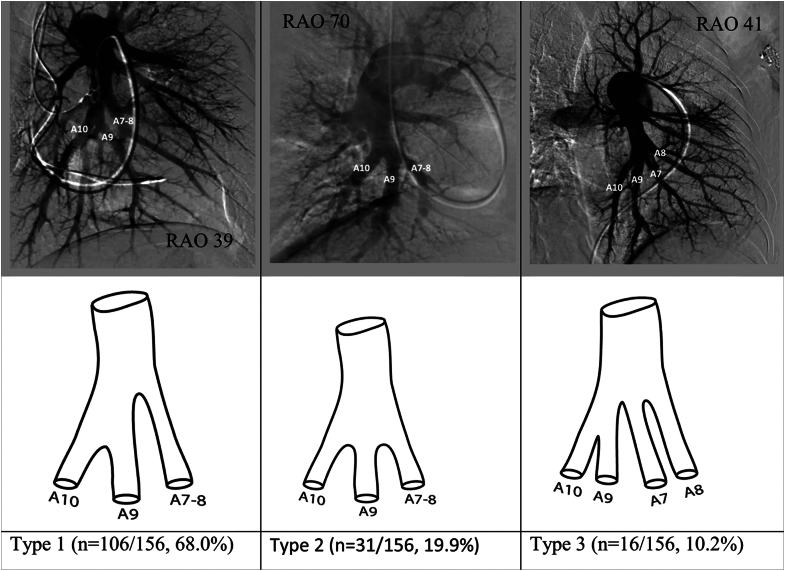
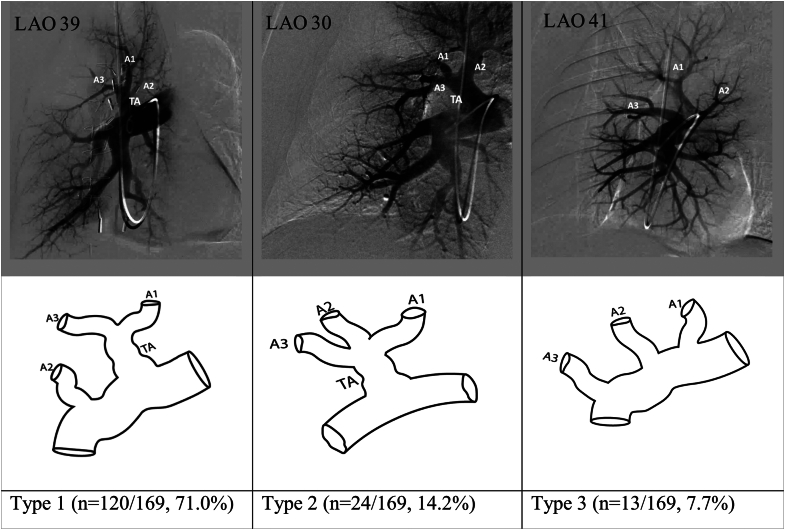
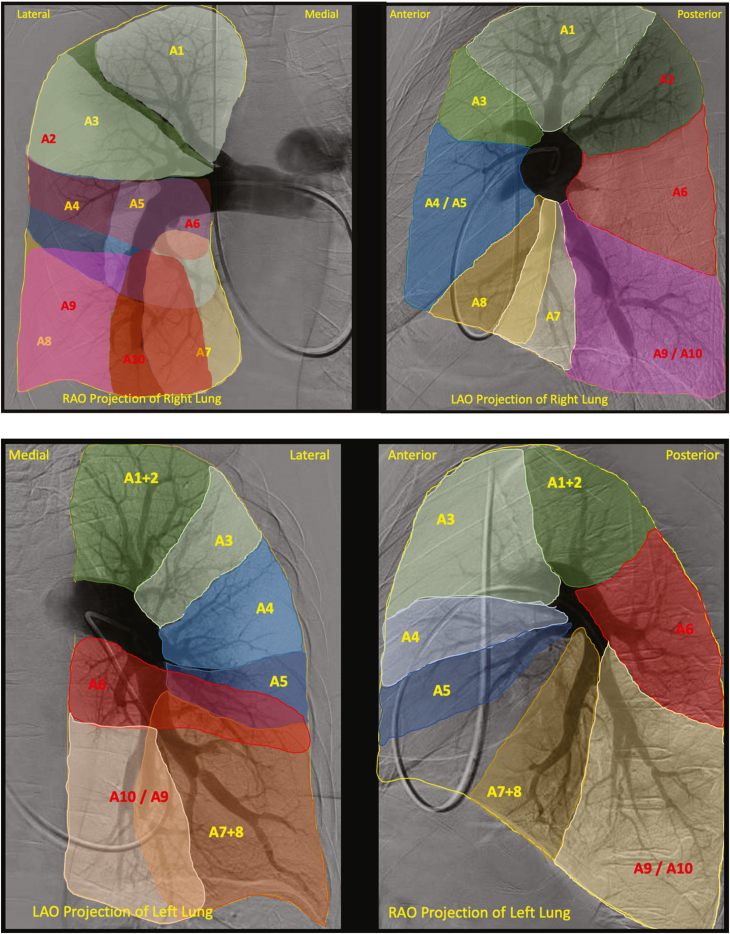
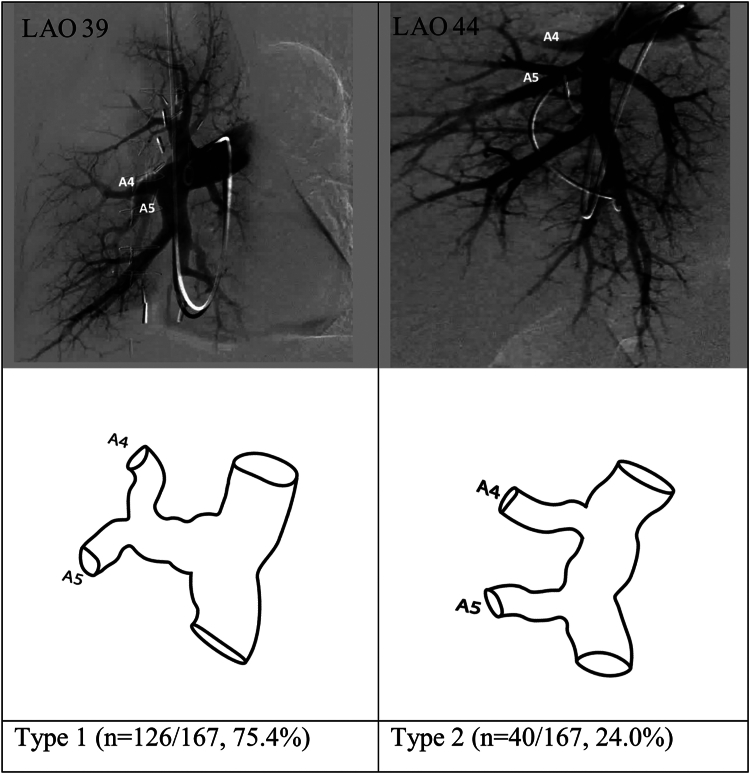
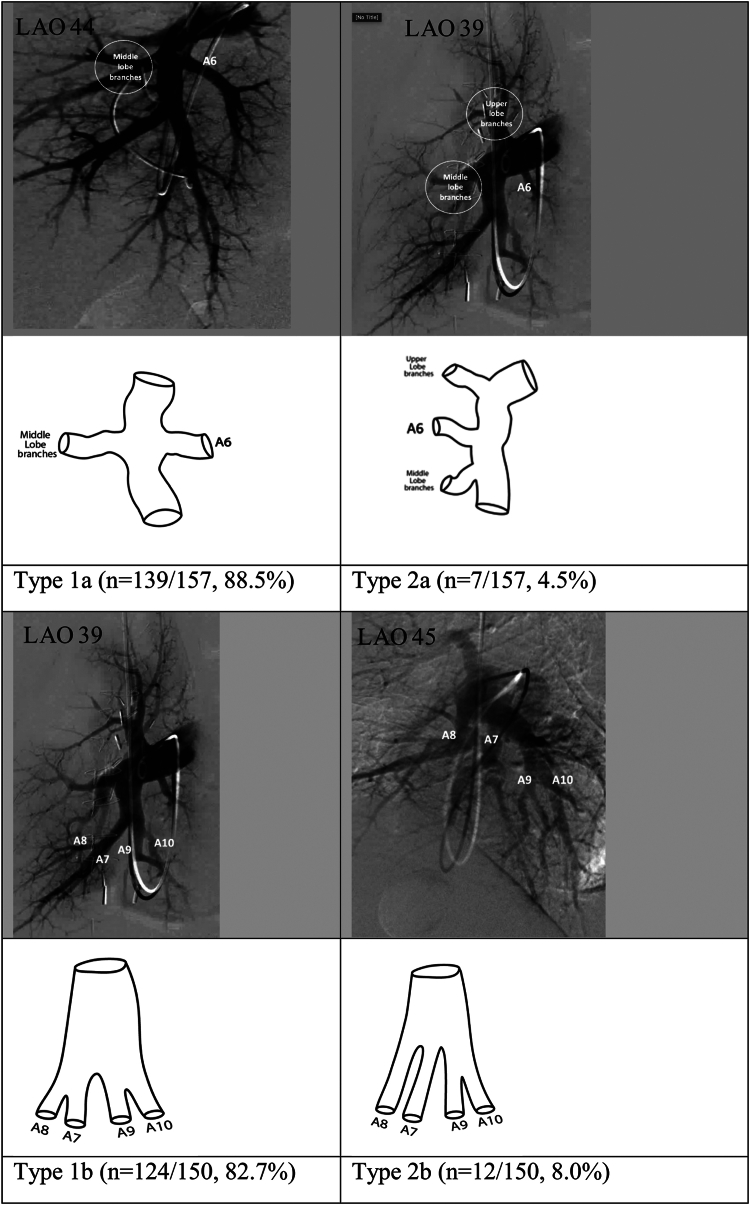
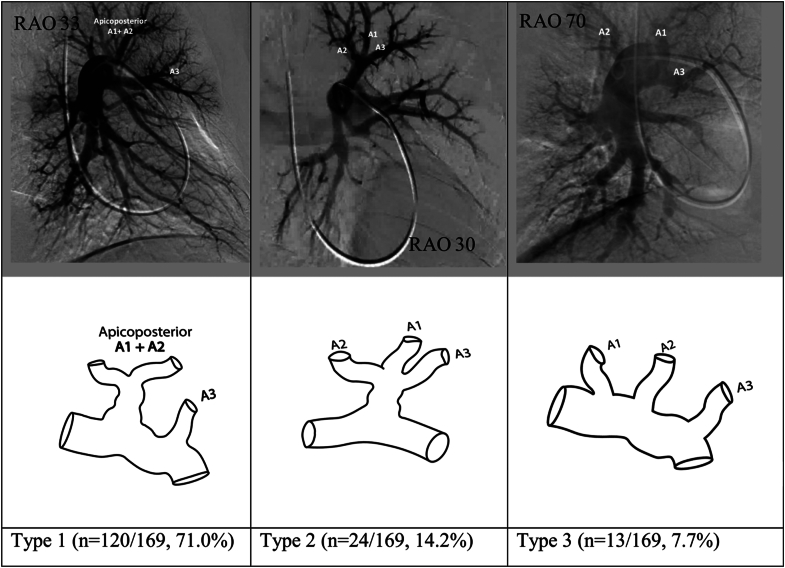
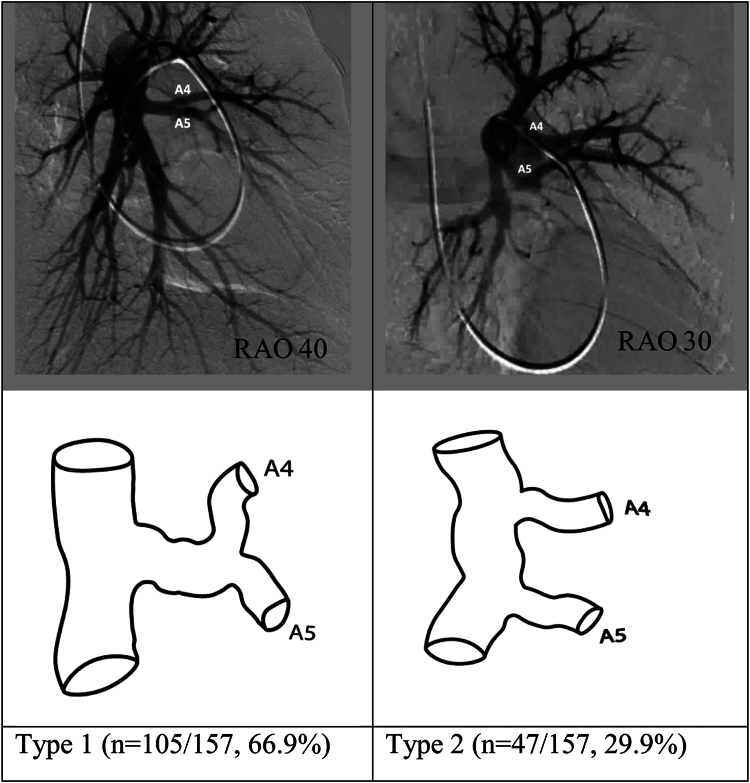
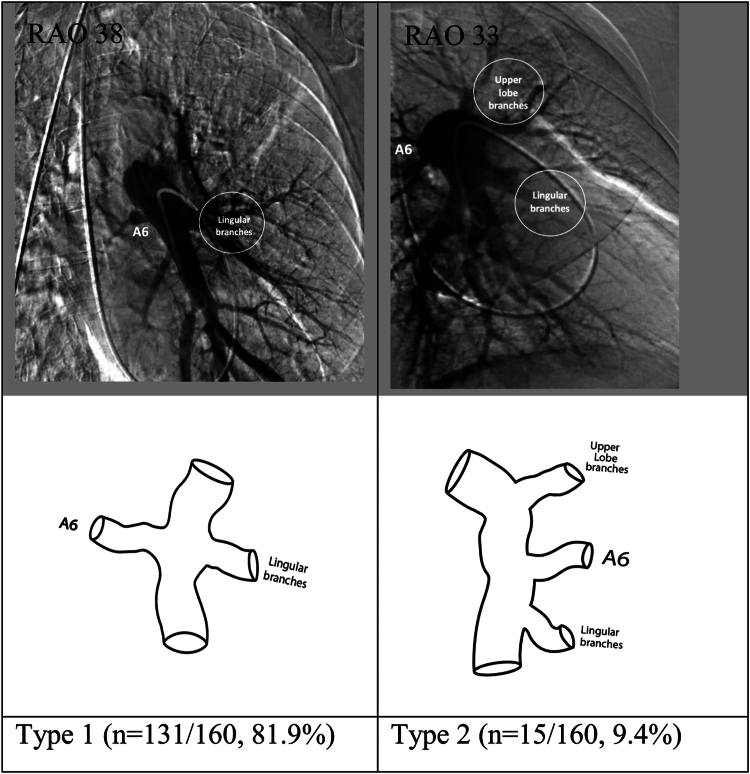
In our study population (age, 59.0 ± 14.8 years, 55.3% female, 71% White), we found several anatomic variations of branches to the different lobes. These included 7 branching patterns in the right upper lobe, 3 in the right middle lobe, and 10 in the right lower lobe (4 patterns for the origin of the superior segmental artery and 6 for the origin of the basilar segmental arteries). On the left side, we found 8 patterns in the left upper lobe, with 5 involving lingular branches, and 9 in the left lower lobe (5 for the origin of the superior segmental artery and 4 for the basilar segmental pulmonary arteries). Although there were many variations, only 2-3 variations for each individual lobe accounted for >90% of the angiograms.
Up to 3 anatomic branching patterns per lobe were noted to account for >90% of pulmonary artery branching variations in this study. This knowledge is not only useful for the interventionalist performing catheter-directed therapies but also for future research efforts that aim to standardize reporting of pulmonary angiographic findings.
基于导管的介入治疗已应用于急性和慢性肺血栓栓塞性疾病。随着这一发展以及对节段性插管的需求,了解肺动脉节段性分支的起源的解剖结构很重要。我们旨在描述不同肺动脉节段性分支起源模式的发生率。
本研究纳入了179例连续接受双侧非选择性有创肺血管造影以评估慢性血栓栓塞性肺动脉高压的患者。
在我们的研究人群(年龄59.0±14.8岁,55.3%为女性,71%为白人)中,我们发现了不同肺叶分支的几种解剖变异。其中右肺上叶有7种分支模式,右肺中叶有3种,右肺下叶有10种(上段动脉起源4种模式,基底段动脉起源6种模式)。在左侧,左肺上叶有8种模式,其中5种涉及舌叶分支,左肺下叶有9种(上段动脉起源5种模式,基底段肺动脉起源4种模式)。虽然存在许多变异,但每个肺叶只有2 - 3种变异占血管造影的>90%。
本研究中,每个肺叶多达3种解剖分支模式占肺动脉分支变异的>90%。这一知识不仅对进行导管导向治疗的介入医生有用,也对未来旨在规范肺血管造影结果报告的研究工作有用。