Minami Naoki, Tsukamoto Shinji, Shimizu Takamasa, Honoki Kanya, Hasegawa Hideo, Masunaga Tomoya, Kido Akira, Errani Costantino, Mavrogenis Andreas F, Tanaka Yasuhito
Department of Orthopaedic Surgery, Nara Medical University, 840 Shijo-cho, Kashihara City, Nara 634-8521, Japan.
Department of Rehabilitation Medicine, Nara Medical University, Nara, Japan.
SICOT J. 2024;10:27. doi: 10.1051/sicotj/2024025. Epub 2024 Aug 13.
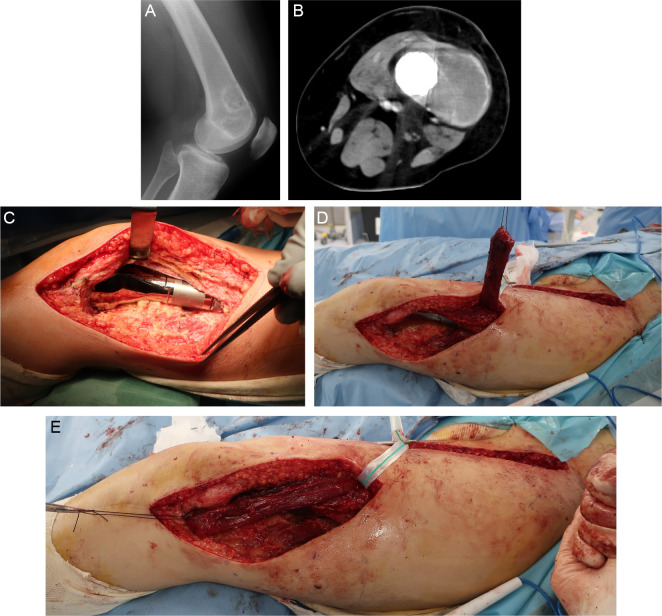
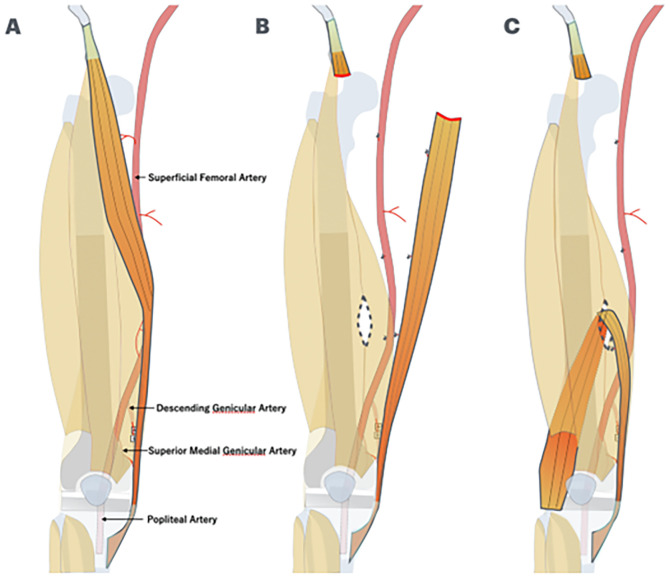
To prevent infection after limb-sparing surgery for primary malignant bone tumors, it is important to cover the megaprosthesis with muscle tissue that has sufficient blood flow. Coverage with a lateral gastrocnemius flap has been reported in cases of distal femoral replacement in which the vastus lateralis and vastus intermedius muscles have been resected; however, the risk of peroneal nerve palsy is reportedly high because the muscle flap passes near the peroneal head. This study was performed to examine the postoperative outcomes of patients with primary malignant bone tumors of the distal femur who underwent wide resection (including the vastus lateralis and vastus intermedius muscles) followed by reconstruction with a megaprosthesis and coverage of the lateral side of the prosthesis with a sartorius muscle flap.
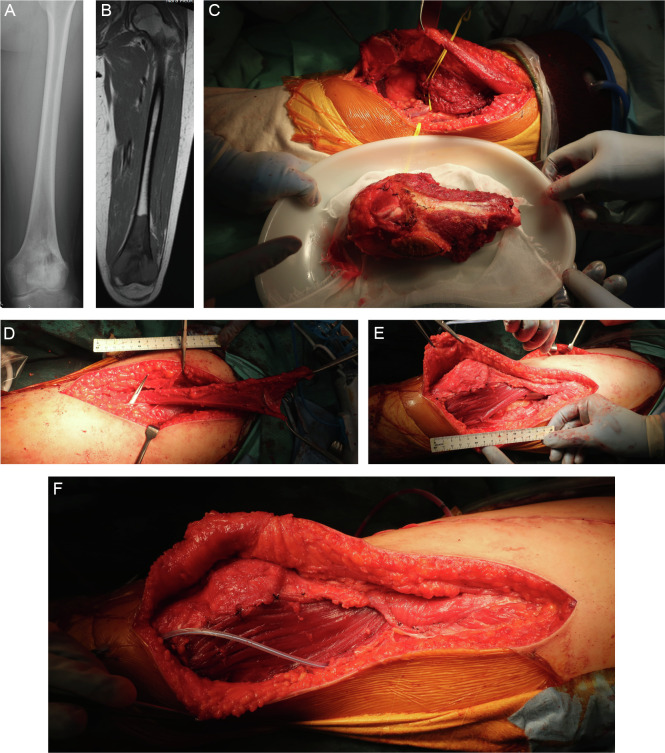
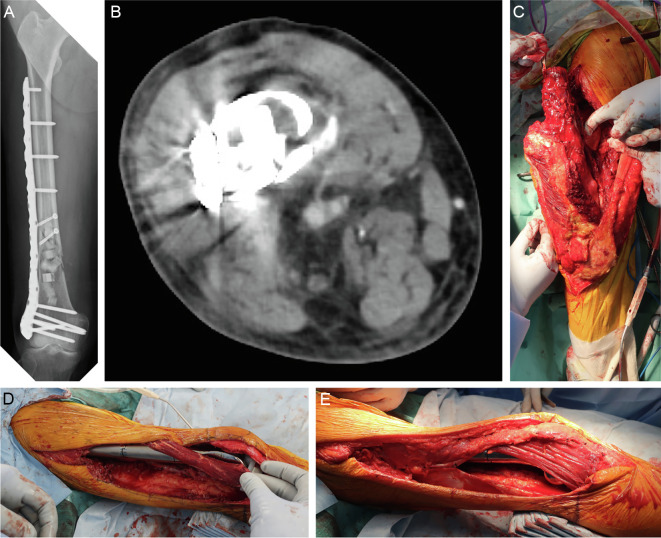
We retrospectively analyzed three patients who underwent reconstruction with a megaprosthesis after wide resection of a primary malignant bone tumor of the distal femur involving the vastus lateralis and vastus intermedius muscles and reconstruction of the soft tissue defect on the lateral side of the prosthesis with a sartorius muscle flap.
The average defect size was 6 × 13 cm, the average time required for a sartorius muscle flap was 100 min, and the average implant coverage was 93%. The average postoperative follow-up period was 35 months, during which no postoperative complications such as infection, skin necrosis, or nerve palsy occurred.
The distally based sartorius muscle flap is easy to elevate in the supine position, has minimal functional loss after harvesting, and has minimal risk of nerve palsy. It can be advocated as the first option for coverage of soft tissue defects lateral to distal femoral replacement.
为预防原发性恶性骨肿瘤保肢手术后的感染,用具有充足血流的肌肉组织覆盖人工关节假体很重要。在股骨远端置换且股外侧肌和股中间肌已被切除的病例中,已有报道采用腓肠外侧肌皮瓣覆盖;然而,据报道腓总神经麻痹的风险较高,因为肌皮瓣经过腓骨头附近。本研究旨在探讨接受股骨远端原发性恶性骨肿瘤广泛切除(包括股外侧肌和股中间肌)、随后用人工关节假体重建并采用缝匠肌皮瓣覆盖假体外侧的患者的术后结局。
我们回顾性分析了3例患者,这些患者在股骨远端原发性恶性骨肿瘤广泛切除(包括股外侧肌和股中间肌)后用人工关节假体进行重建,并采用缝匠肌皮瓣修复假体外侧的软组织缺损。
平均缺损大小为6×13厘米,缝匠肌皮瓣平均所需时间为100分钟,平均植入物覆盖率为93%。术后平均随访期为35个月,在此期间未发生感染、皮肤坏死或神经麻痹等术后并发症。
以远端为蒂的缝匠肌皮瓣在仰卧位易于掀起,切取后功能损失最小,神经麻痹风险最低。它可被推荐为股骨远端置换外侧软组织缺损覆盖的首选方案。