Department of Surgery, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin, Korea.
Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
JAMA Surg. 2024 Oct 1;159(10):1177-1186. doi: 10.1001/jamasurg.2024.2977.
While nipple-sparing mastectomy (NSM) for breast cancer was only performed using the open method in the past, its frequency using endoscopic and robotic surgical instruments has been increasing rapidly. However, there are limited studies regarding postoperative complications and the benefits and drawbacks of minimal access NSM (M-NSM) compared with conventional NSM (C-NSM).
To examine the differences in postoperative complications between C-NSM and M-NSM.
DESIGN, SETTING, PARTICIPANTS: This was a retrospective multicenter cohort study enrolling 1583 female patients aged 19 years and older with breast cancer who underwent NSM at 21 university hospitals in Korea between January 2018 and December 2020. Those with mastectomy without preserving the nipple-areolar complex (NAC), clinical or pathological malignancy in the NAC, inflammatory breast cancer, breast cancer infiltrating the chest wall or skin, metastatic breast cancer, or insufficient medical records were excluded. Data were analyzed from November 2021 to March 2024.
M-NSM or C-NSM.
Clinicopathological factors and postoperative complications within 3 months of surgery were assessed. Statistical analyses, including logistic regression, were used to identify the factors associated with complications.
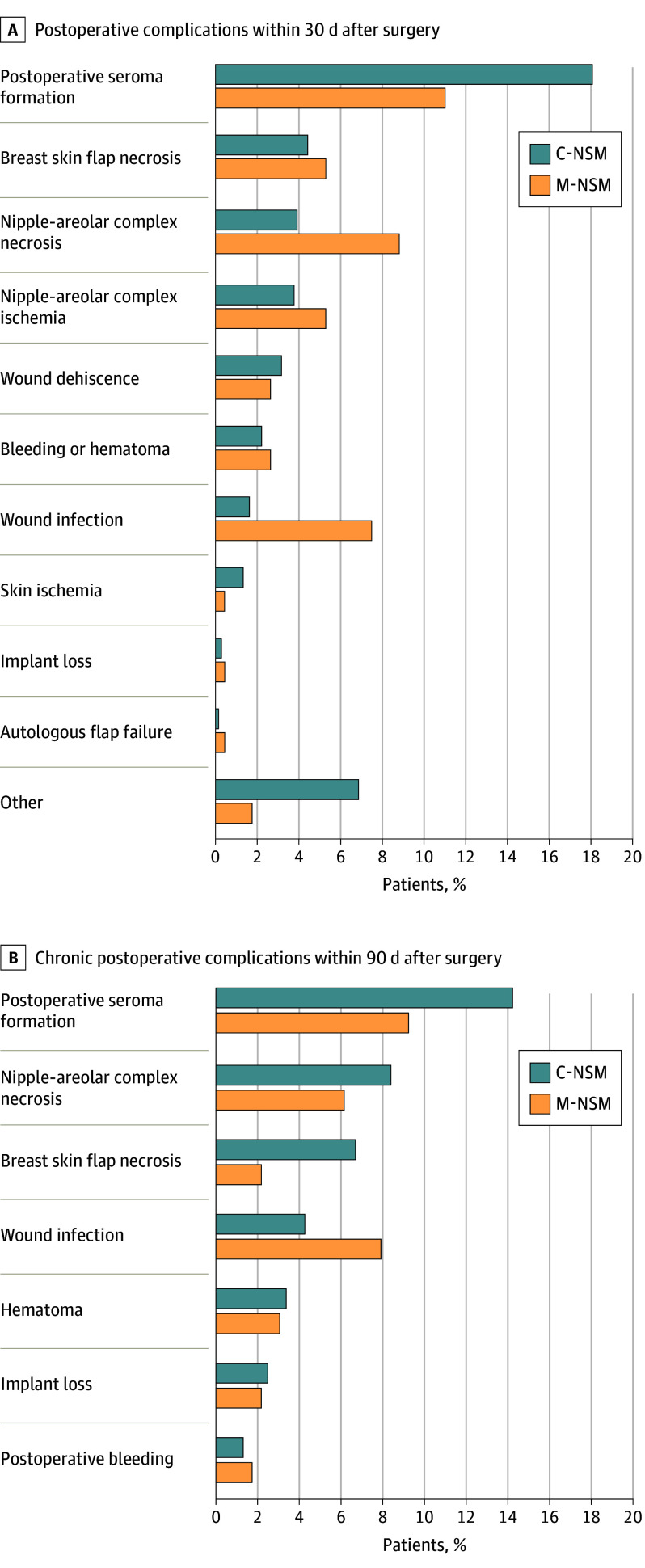
There were 1356 individuals (mean [SD] age, 45.47 [8.56] years) undergoing C-NSM and 227 (mean [SD] age, 45.41 [7.99] years) undergoing M-NSM (35 endoscopy assisted and 192 robot assisted). There was no significant difference between the 2 groups regarding short- and long-term postoperative complications (<30 days: C-NSM, 465 of 1356 [34.29%] vs M-NSM, 73 of 227 [32.16%]; P = .53; <90 days: C-NSM, 525 of 1356 [38.72%] vs M-NSM, 73 of 227 [32.16%]; P = .06). Nipple-areolar complex necrosis was more common in the long term after C-NSM than M-NSM (C-NSM, 91 of 1356 [6.71%] vs M-NSM, 5 of 227 [2.20%]; P = .04). Wound infection occurred more frequently after M-NSM (C-NSM, 58 of 1356 [4.28%] vs M-NSM, 18 of 227 [7.93%]; P = .03). Postoperative seroma occurred more frequently after C-NSM (C-NSM, 193 of 1356 [14.23%] vs M-NSM, 21 of 227 [9.25%]; P = .04). Mild or severe breast ptosis was a significant risk factor for nipple or areolar necrosis (odds ratio [OR], 4.75; 95% CI, 1.66-13.60; P = .004 and OR, 8.78; 95% CI, 1.88-41.02; P = .006, respectively). Conversely, use of a midaxillary, anterior axillary, or axillary incision was associated with a lower risk of necrosis (OR for other incisions, 32.72; 95% CI, 2.11-508.36; P = .01). Necrosis occurred significantly less often in direct-to-implant breast reconstruction compared to other breast reconstructions (OR, 2.85; 95% CI, 1.11-7.34; P = .03).
The similar complication rates between C-NSM and M-NSM demonstrates that both methods were equally safe, allowing the choice to be guided by patient preferences and specific needs.
过去,保乳乳房切除术(NSM)仅采用开放式方法进行,但其使用内窥镜和机器人手术器械的频率迅速增加。然而,与传统 NSM(C-NSM)相比,关于微创手术 NSM(M-NSM)的术后并发症、益处和缺点的研究有限。
研究 C-NSM 和 M-NSM 之间术后并发症的差异。
设计、地点、参与者:这是一项回顾性多中心队列研究,纳入了 2018 年 1 月至 2020 年 12 月期间在韩国 21 所大学医院接受 NSM 的 1583 名年龄在 19 岁及以上的乳腺癌女性患者。排除乳房切除术不保留乳头乳晕复合体(NAC)、NAC 有临床或病理恶性、炎性乳腺癌、乳房癌浸润胸壁或皮肤、转移性乳腺癌或病历记录不充分的患者。数据于 2021 年 11 月至 2024 年 3 月进行分析。
M-NSM 或 C-NSM。
评估手术 3 个月内的临床病理因素和术后并发症。使用逻辑回归等统计分析方法确定与并发症相关的因素。
有 1356 名患者(平均年龄[标准差],45.47[8.56]岁)接受了 C-NSM,227 名患者(平均年龄[标准差],45.41[7.99]岁)接受了 M-NSM(35 名接受内窥镜辅助手术,192 名接受机器人辅助手术)。两组在短期和长期术后并发症方面无显著差异(<30 天:C-NSM,1356 例中的 465 例[34.29%] vs M-NSM,227 例中的 73 例[32.16%];P=0.53;<90 天:C-NSM,1356 例中的 525 例[38.72%] vs M-NSM,227 例中的 73 例[32.16%];P=0.06)。与 M-NSM 相比,C-NSM 后乳头乳晕复合体坏死更为常见(长期:C-NSM,1356 例中的 91 例[6.71%] vs M-NSM,227 例中的 5 例[2.20%];P=0.04)。M-NSM 后发生伤口感染的频率更高(C-NSM,1356 例中的 58 例[4.28%] vs M-NSM,227 例中的 18 例[7.93%];P=0.03)。C-NSM 后发生术后血清肿的频率更高(C-NSM,1356 例中的 193 例[14.23%] vs M-NSM,227 例中的 21 例[9.25%];P=0.04)。轻度或重度乳房下垂是乳头或乳晕坏死的显著危险因素(比值比[OR],4.75;95%置信区间[CI],1.66-13.60;P=0.004 和 OR,8.78;95% CI,1.88-41.02;P=0.006)。相反,采用腋前线、前腋或腋部切口与坏死风险较低相关(其他切口的 OR,32.72;95% CI,2.11-508.36;P=0.01)。与其他乳房重建相比,直接植入乳房重建中坏死的发生率显著降低(OR,2.85;95% CI,1.11-7.34;P=0.03)。
C-NSM 和 M-NSM 的相似并发症发生率表明这两种方法同样安全,可以根据患者的偏好和特定需求来选择。