Department of Neurology, University Regional Hospital Centre of Nancy, Nancy, France.
Nutrition-Genetics and Exposure to Environmental Risks, UMR 1256, INSERM, University of Lorraine, Nancy, France.
Eur J Neurol. 2024 Dec;31(12):e16432. doi: 10.1111/ene.16432. Epub 2024 Aug 16.
Our objective was to define phenotypes of non-lesional late-onset epilepsy (NLLOE) depending on its presumed aetiology and to determine their seizure and cognitive outcomes at 12 months.
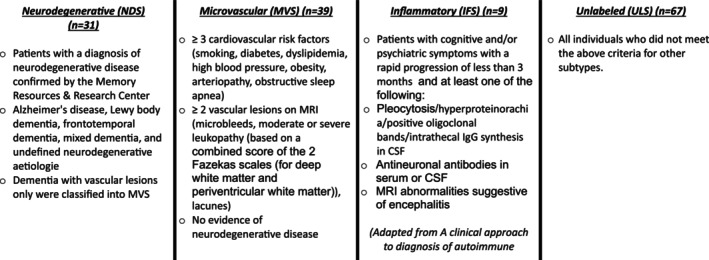
In all, 146 newly diagnosed NLLOE patients, >50 years old, were prospectively included and categorized by four presumed aetiological subtypes: neurodegenerative subtype (patients with a diagnosis of neurodegenerative disease) (n = 31), microvascular subtype (patients with three or more cardiovascular risk factors and two or more vascular lesions on MRI) (n = 39), inflammatory subtype (patient meeting international criteria for encephalitis) (n = 9) and unlabelled subtype (all individuals who did not meet the criteria for other subtypes) (n = 67). Cognitive outcome was determined by comparing for each patient the proportion of preserved/altered scores between initial and second neuropsychological assessment.
The neurodegenerative subtype had the most severe cognitive profile at diagnosis with cognitive complaint dating back several years. The microvascular subtype was mainly evaluated through the neurovascular emergency pathway. Their seizures were characterized by transient phasic disorders. Inflammatory subtype patients were the youngest. They presented an acute epilepsy onset with high rate of focal status epilepticus. The unlabelled subtype presented fewer comorbidities with fewer lesions on brain imaging. The neurodegenerative subtype had the worst seizure and cognitive outcomes. In other groups, seizure control was good under antiseizure medication (94.7% seizure-free) and cognitive performance was stabilized or even improved.
This new characterization of NLLOE phenotypes raises questions regarding the current International League Against Epilepsy aetiological classification which does not individualize neurodegenerative and microvascular aetiology per se.
本研究旨在根据推测的病因对非病灶性晚发性癫痫(NLLOE)的表型进行定义,并确定其在 12 个月时的发作和认知结局。
共前瞻性纳入 146 例新诊断的 NLLOE 患者(年龄>50 岁),并根据四种推测的病因亚型进行分类:神经退行性亚型(有神经退行性疾病诊断的患者)(n=31)、微血管亚型(有三个或更多心血管危险因素和两个或更多 MRI 血管病变的患者)(n=39)、炎症性亚型(符合国际脑炎标准的患者)(n=9)和未标记亚型(不符合其他亚型标准的所有患者)(n=67)。认知结局通过比较每位患者初始和第二次神经心理学评估之间保留/改变分数的比例来确定。
神经退行性亚型在诊断时认知状况最严重,认知主诉可追溯数年。微血管亚型主要通过神经血管急诊途径进行评估。他们的发作特点是短暂的阶段性障碍。炎症性亚型患者年龄最小。他们表现为急性癫痫发作,局灶性癫痫持续状态的发生率较高。未标记亚型的合并症较少,脑成像上的病变较少。神经退行性亚型的发作和认知结局最差。在其他组中,抗癫痫药物(94.7%无发作)控制发作良好,认知表现稳定甚至改善。
这种对 NLLOE 表型的新特征描述引发了对当前国际抗癫痫联盟病因分类的质疑,该分类本身并未对神经退行性和微血管病因进行个体化分类。