Yazhini Shanmugam, Venkatraman Rajagopalan, Kandan Karthik
Anaesthesiology, SRM Medical College Hospital and Research Centre, Chennai, IND.
Cureus. 2024 Jul 17;16(7):e64732. doi: 10.7759/cureus.64732. eCollection 2024 Jul.
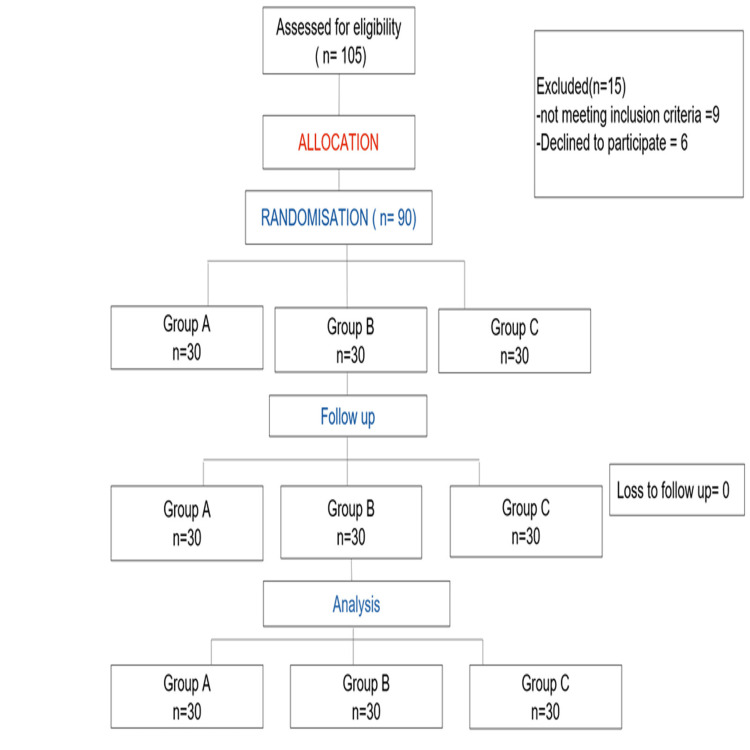
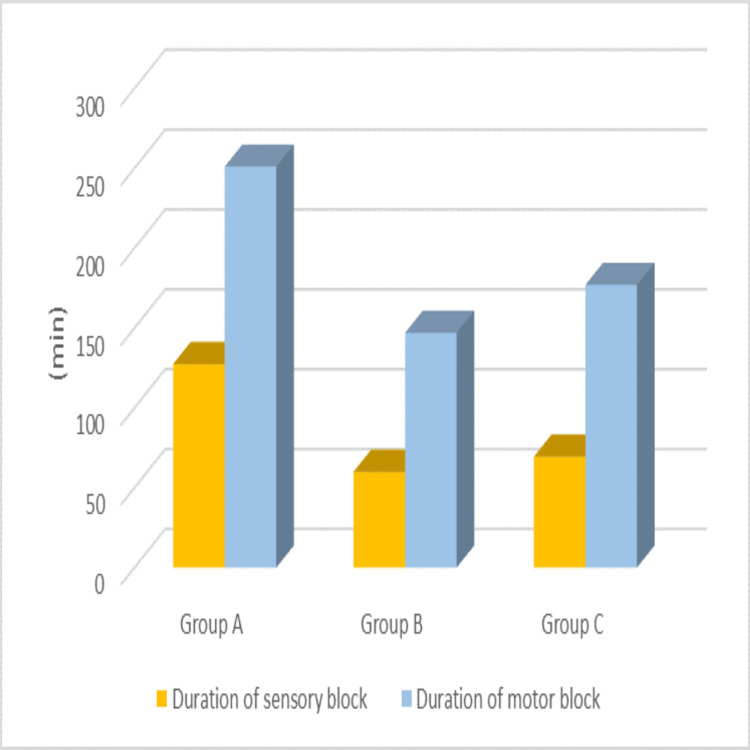
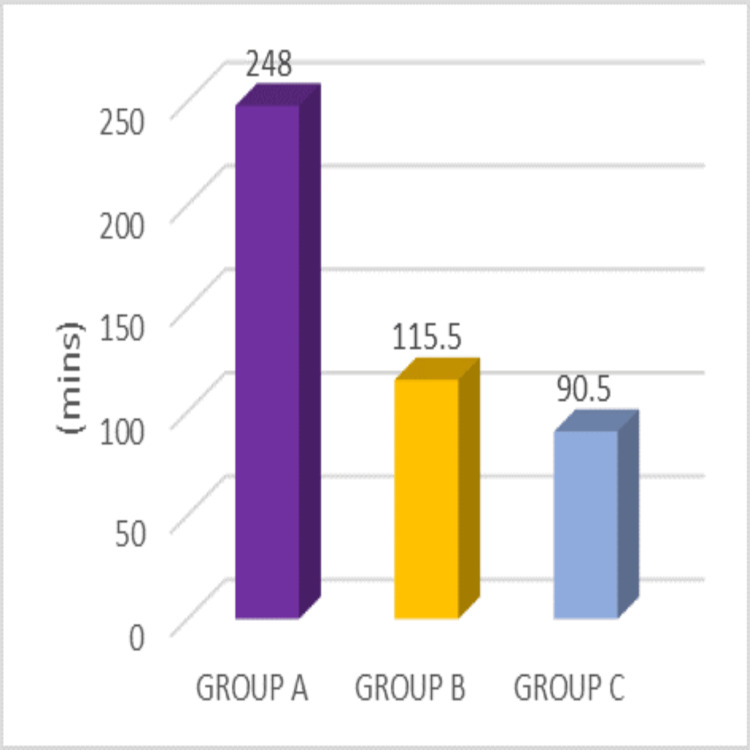
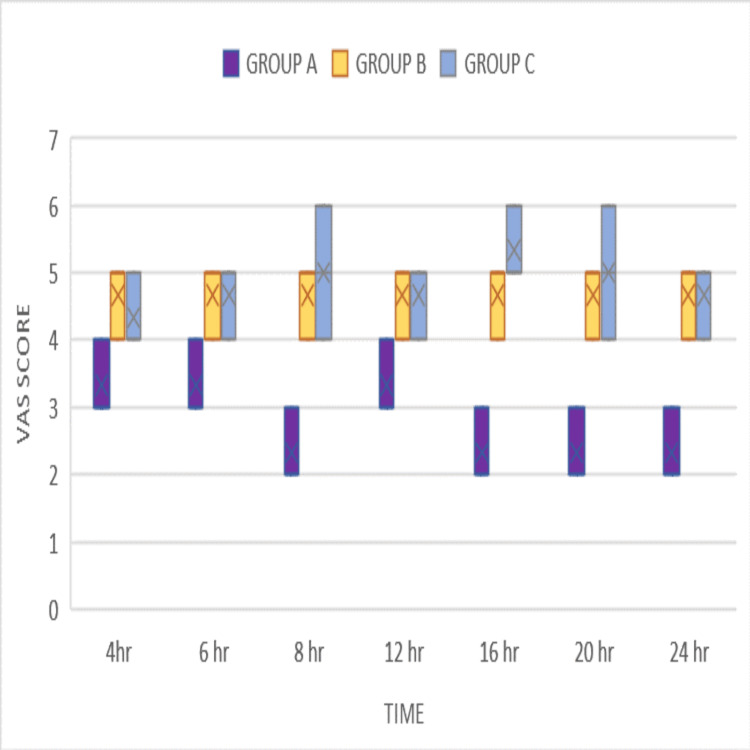
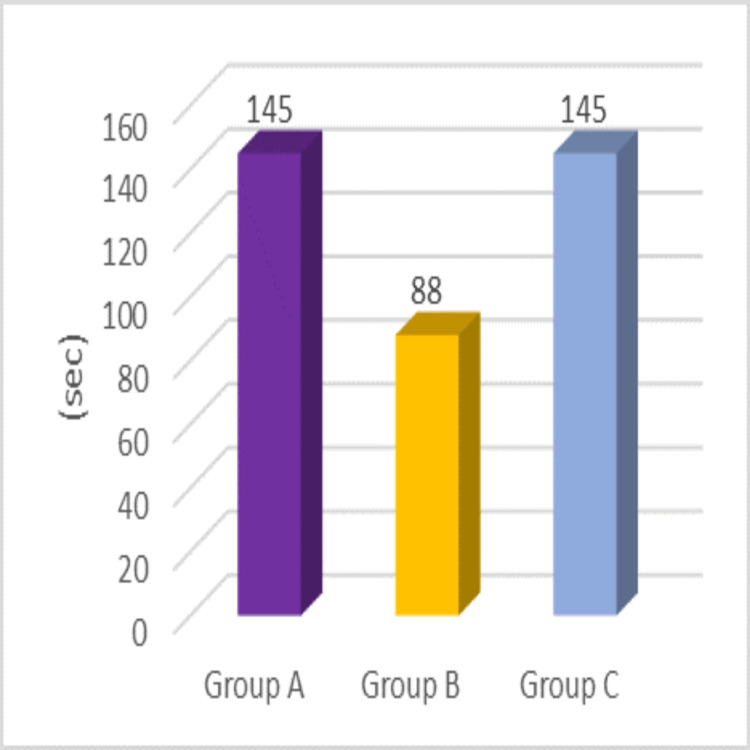
Background and objectives Spinal anesthesia stands as a cornerstone for patients undergoing lower segment cesarean section (LSCS), offering advantages like faster onset and high block density. Levobupivacaine, known for its high potency and long-acting nature, has a slower onset. The safety of intrathecal fentanyl or midazolam is evaluated as an adjuvant to levobupivacaine in parturients. This study aims to compare the duration of postoperative analgesia provided by fentanyl or midazolam added to 0.5% hyperbaric levobupivacaine in elective cesarean sections. Secondary objectives include evaluating the onset and duration of sensory and motor blockade and the incidence of nausea and vomiting. Identifying the more effective adjuvant will help optimize spinal anesthesia protocols, improve postoperative outcomes, and enhance patient comfort and recovery. Methods This study was conducted at SRM Medical College Hospital and Research Centre, Chennai, India, over six months (May 1, 2023, to October 1, 2023). A total of 90 patients undergoing elective LSCS received spinal anesthesia in a prospective randomized double-blinded controlled trial. Patients were allocated to three groups: Group A received levobupivacaine with fentanyl, Group B received levobupivacaine with midazolam, and Group C received levobupivacaine with normal saline. Block characteristics, postoperative analgesia, hemodynamic stability, and complications were assessed. Assessments were conducted at specified time points: intraoperatively, every five minutes for the first 30 minutes, every 10 minutes for the next hour, every two hours for six hours, and every four hours up to 24 hours postoperatively. Statistical analysis utilized one-way analysis of variance (ANOVA). Results Group B (levobupivacaine with midazolam) exhibited a shorter time to sensory block onset (88 seconds) compared to Groups A and C (both 145 seconds) (p < 0.001). Group A (levobupivacaine with fentanyl) showed a shorter time to maximum motor block (p = 0.045) than Groups B and C. The sensory block duration was significantly longer in Group A (127.5 minutes) compared to Group B (60 minutes) and Group C (69 minutes) (p < 0.001). Motor block duration was also prolonged in Group A (251 minutes) compared to Group B (147 minutes) and Group C (177 minutes) (p = 0.045). The first analgesic requirement was delayed in Group A (248 minutes), whereas Groups B (115 minutes) and C (90 minutes) (p < 0.001) required more frequent analgesia. Group A experienced a higher incidence of postoperative nausea and vomiting. Conclusion Midazolam accelerated sensory block onset, while fentanyl prolonged anesthesia duration without significantly affecting motor block. Fentanyl delayed the first analgesic requirement, whereas midazolam reduced postoperative nausea, vomiting, and shivering.
背景与目的 脊髓麻醉是下段剖宫产术(LSCS)患者的基石,具有起效快和阻滞密度高的优点。左旋布比卡因以其高效能和长效性著称,但起效较慢。本研究评估鞘内注射芬太尼或咪达唑仑作为左旋布比卡因辅助药物在产妇中的安全性。本研究旨在比较在择期剖宫产术中,芬太尼或咪达唑仑添加到0.5%重比重左旋布比卡因中所提供的术后镇痛持续时间。次要目标包括评估感觉和运动阻滞的起效时间和持续时间以及恶心和呕吐的发生率。确定更有效的辅助药物将有助于优化脊髓麻醉方案、改善术后结局并提高患者舒适度和恢复情况。方法 本研究在印度钦奈的SRM医学院医院和研究中心进行,为期六个月(2023年5月1日至2023年10月1日)。在一项前瞻性随机双盲对照试验中,共有90例接受择期LSCS的患者接受脊髓麻醉。患者被分为三组:A组接受左旋布比卡因加芬太尼,B组接受左旋布比卡因加咪达唑仑,C组接受左旋布比卡因加生理盐水。评估阻滞特征、术后镇痛、血流动力学稳定性和并发症。在特定时间点进行评估:术中,前30分钟每5分钟一次;接下来的1小时每10分钟一次;6小时内每2小时一次;术后24小时内每4小时一次。统计分析采用单因素方差分析(ANOVA)。结果 与A组和C组(均为秒)相比B组(左旋布比卡因加咪达唑仑)感觉阻滞起效时间更短(88秒)(p <0.001)A组(左旋布比卡因加芬太尼)达到最大运动阻滞时间比B组和C组短(p =0.045)。与B组(60分钟)和C组(69分钟)相比,A组的感觉阻滞持续时间明显更长(127.5分钟)(p <0.001)。与B组(147分钟)和C组(177分钟)相比,A组的运动阻滞持续时间也延长(251分钟)(p =0.045)。A组首次镇痛需求延迟,而B组(115分钟)和C组(90分钟)(p <0.001)需要更频繁的镇痛。A组术后恶心和呕吐的发生率更高。结论 咪达唑仑加速了感觉阻滞的起效,而芬太尼延长了麻醉持续时间,且对运动阻滞无显著影响。芬太尼延迟了首次镇痛需求,而咪达唑仑减少了术后恶心、呕吐和寒战。