Badge Rohit, Rathore Vinay, Aggarwal Jyoti
Department of Nephrology, AIIMS Raipur, Chhattisgarh, India.
Indian J Nephrol. 2024 Jul-Aug;34(4):385-387. doi: 10.25259/ijn_363_23. Epub 2024 May 9.
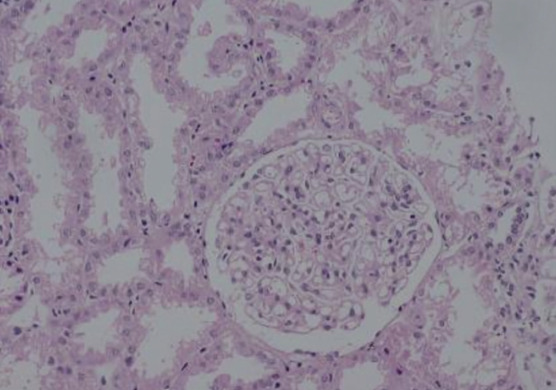
Parasitic infections like filariasis are uncommon causes of secondary membranous nephropathy (MN) which requires serological tests to detect circulating Wuchereria bancrofti antigens for its diagnosis or the identification of microfilariae in the capillary lumen on kidney biopsy. The immunochromatographic card tests is simple, non invasive and has high sensitivity and specificity. We report a case of 30 year old lady who presented to us with nephrotic syndrome which on kidney biopsy showed features of membranous nephropathy with negative staining for Anti PLA2R, THSD7A and exostosin. A thorough workup was done to find out any secondary cause of MN where she was found positive with filiarial antibody test. Hence, a diagnosis of secondary membranous pattern nephropathy was considered for which she was treated with diethylcarbamazine (DEC) and other supportive medications which on follow up showed marked resolution of proteinuria.
像丝虫病这样的寄生虫感染是继发性膜性肾病(MN)的罕见病因,其诊断需要进行血清学检测以检测循环中的班氏吴策线虫抗原,或在肾活检时识别毛细血管腔内的微丝蚴。免疫层析卡检测简单、无创,具有高灵敏度和特异性。我们报告一例30岁女性,因肾病综合征前来就诊,肾活检显示膜性肾病特征,抗磷脂酶A2受体(Anti PLA2R)、血小板反应蛋白7A(THSD7A)和外切糖苷酶染色均为阴性。进行了全面检查以寻找MN的任何继发性病因,结果发现她的丝虫抗体检测呈阳性。因此,考虑诊断为继发性膜性肾病样型,为此她接受了乙胺嗪(DEC)和其他支持性药物治疗,随访显示蛋白尿明显消退。