Kurnikowski Amelie, Werzowa Johannes, Hödlmoser Sebastian, Krenn Simon, Paschen Christopher, Mussnig Sebastian, Tura Andrea, Harreiter Jürgen, Krebs Michael, Song Peter X K, Eller Kathrin, Pascual Julio, Budde Klemens, Hecking Manfred, Schwaiger Elisabeth
Division of Nephrology and Dialysis, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria.
Department of Epidemiology, Center for Public Health, Medical University of Vienna, Vienna, Austria.
Kidney Med. 2024 Jun 21;6(8):100860. doi: 10.1016/j.xkme.2024.100860. eCollection 2024 Aug.
RATIONALE & OBJECTIVES: Hyperglycemia is frequently observed early after transplantation and associated with development of post-transplant diabetes mellitus (PTDM). Here, we assessed continuous subcutaneous insulin infusion (CSII) targeting afternoon hyperglycemia.
Open-label randomized parallel 3-arm design.
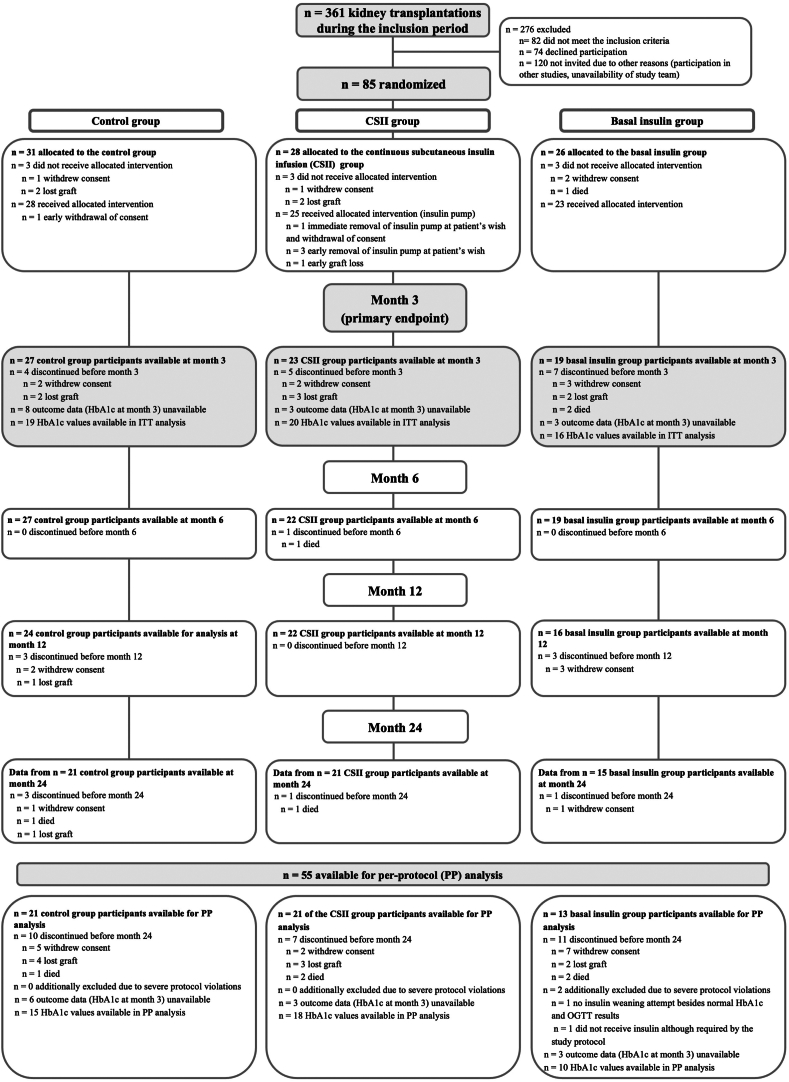
SETTINGS & PARTICIPANTS: In total, 85 kidney transplant recipients without previous diabetes diagnosis were randomized to postoperative CSII therapy, basal insulin, or control.
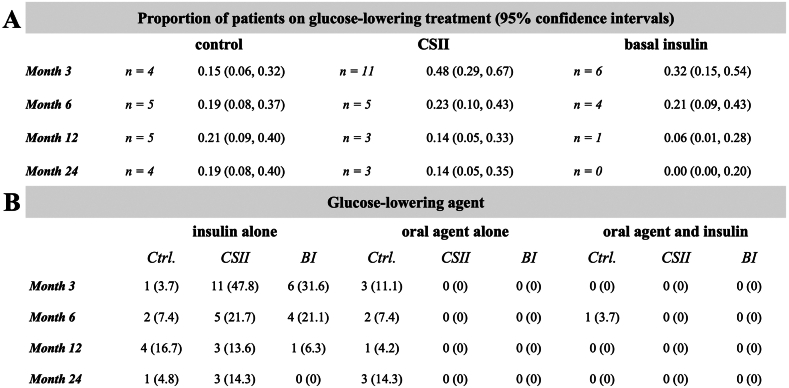
Insulin was to be initiated at afternoon capillary blood glucose level of ≥140 mg/dL (7.8 mmol/L; CSII and basal insulin) or fasting plasma glucose level of ≥200 mg/dL (11.1 mmol/L; control).
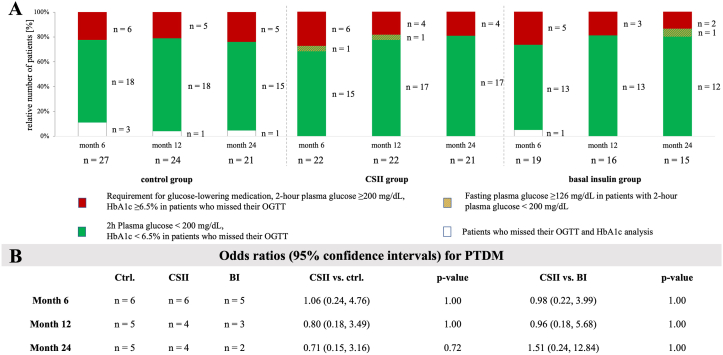
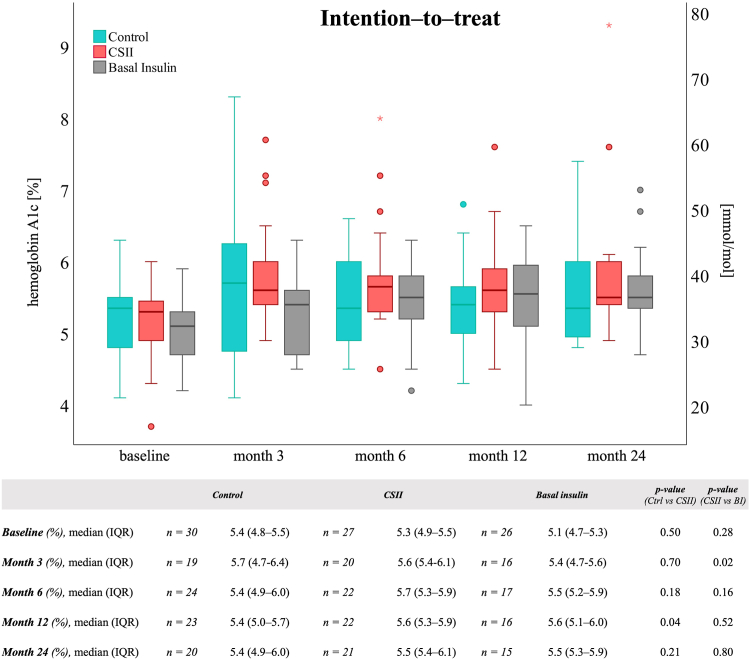
Hemoglobin A1c (HbA1c) levels at 3 months post-transplant (primary endpoint). PTDM assessed using oral glucose tolerance test at 12 and 24 months.
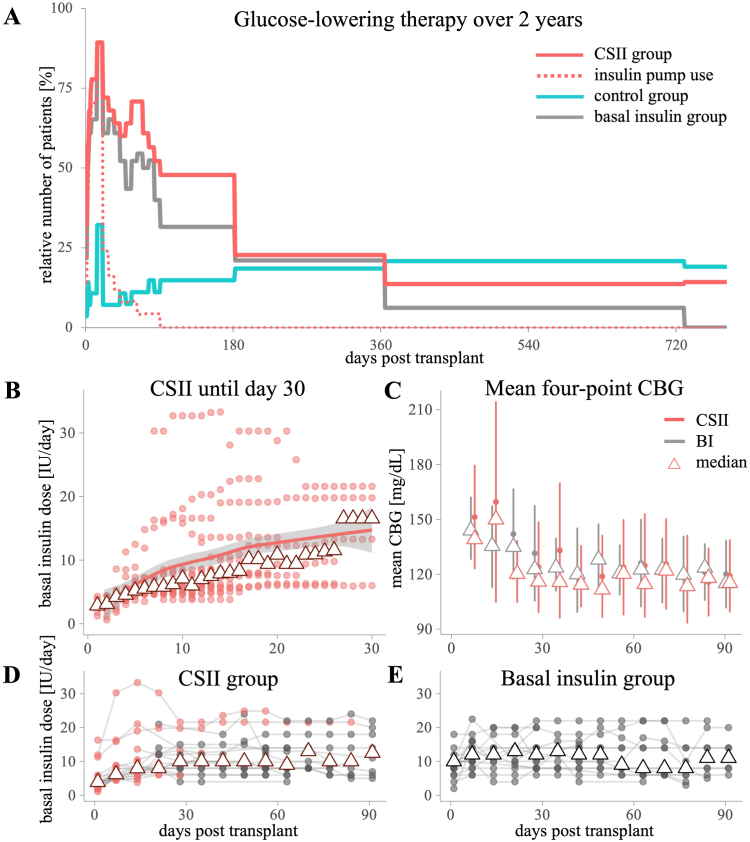
CSII therapy lasted until median day 18 and maximum day 88. The median HbA1c value at month 3 was 5.6% (38 mmol/mol) in the CSII group versus 5.7% (39 mmol/mol) in the control group ( = 0.70) and 5.4% (36 mmol/mol) in the basal insulin group ( = 0.02). At months 12 and 24, the odds for PTDM were similar compared with the control group (odds ratios [95% confidence intervals], 0.80 [0.18-3.49] and 0.71 [0.15-3.16], respectively) and the basal insulin group (0.96 [0.18-5.68] and 1.51 [0.24-12.84], respectively). Mild hypoglycemia events occurred in the CSII and the basal insulin groups.
This study is limited by outdated insulin pump technology, frequent discontinuations of CSII, a complex protocol, and concerns regarding reliability of HbA1c measurements.
CSII therapy was not superior at reducing HbA1c levels at month 3 or PTDM prevalence at months 12 and 24 compared with the control or basal insulin group.
移植后早期经常出现高血糖,且与移植后糖尿病(PTDM)的发生有关。在此,我们评估了针对下午高血糖的持续皮下胰岛素输注(CSII)。
开放标签随机平行三组设计。
总共85名既往未诊断糖尿病的肾移植受者被随机分为术后CSII治疗组、基础胰岛素组或对照组。
当下午毛细血管血糖水平≥140mg/dL(7.8mmol/L;CSII和基础胰岛素组)或空腹血糖水平≥200mg/dL(11.1mmol/L;对照组)时开始使用胰岛素。
移植后3个月时的糖化血红蛋白(HbA1c)水平(主要终点)。在12个月和24个月时使用口服葡萄糖耐量试验评估PTDM。
CSII治疗持续至中位数第18天和最长第88天。CSII组第3个月的HbA1c中位数为5.6%(38mmol/mol),对照组为5.7%(3mmol/mol)(P = 0.70),基础胰岛素组为5.4%(36mmol/mol)(P = 0.02)。在12个月和24个月时,与对照组相比,PTDM的几率相似(优势比[95%置信区间]分别为0.80[0.18 - 3.49]和0.71[0.15 - 3.16]),与基础胰岛素组相比也相似(分别为0.96[0.18 - 5.68]和1.51[0.24 - 12.84])。CSII组和基础胰岛素组均发生了轻度低血糖事件。
本研究受胰岛素泵技术过时、CSII频繁中断、方案复杂以及HbA1c测量可靠性问题的限制。
与对照组或基础胰岛素组相比,CSII治疗在降低第3个月的HbA1c水平或第12个月和24个月的PTDM患病率方面并无优势。