Uchida Lisa, Jones Rachel B, Smith Rona M, Nodale Marianna, Bond Simon, Loechel Claudia, King Maria, Luqmani Raashid, Gray David, Barrett Joe, Jayne David R W
Department of Medicine, University of Cambridge, Cambridge, UK.
Vasculitis and Lupus Clinic, Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK.
Rheumatol Adv Pract. 2024 Aug 6;8(3):rkae090. doi: 10.1093/rap/rkae090. eCollection 2024.
Rituximab is used for remission induction and the prevention of relapse in anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV). This study evaluated the incidence of safety events and compared time to first serious adverse event (SAE) between a rituximab cohort and a cohort treated with non-rituximab therapies in a real-life setting.
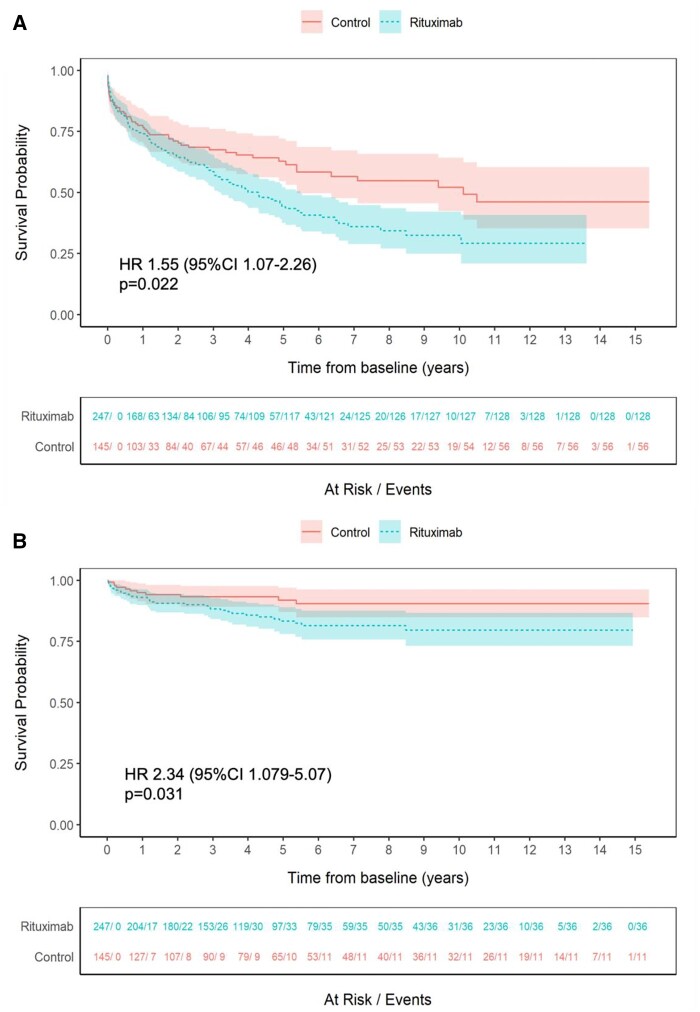
Rituximab surveillance study in vasculitis was a retrospective observational study of patients with AAV who received rituximab (MabThera) or other treatments between 2003 and 2017 at a specialist vasculitis clinic. The primary endpoint was time to first SAE.
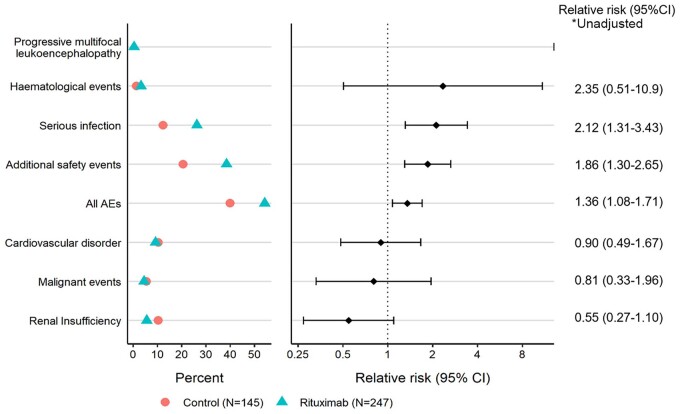
392 patients were enrolled: 247 in the rituximab and 145 in the control cohorts with a total follow up of 2217 person-years (mean study duration 5.7 years). Mean age was 61 years, 77% had granulomatosis with polyangiitis (GPA). There were differences in baseline characteristics (disease duration and prior immunosuppressive use) between groups. 134/247 patients (54%) in the rituximab and 58/145 (40%) of controls experienced at least one SAE. Time to first SAE was shorter in the rituximab group (hazard ratio (HR) 1.55, 95% CI 1.07-2.26, = 0.022). Predictors of first SAE were higher vasculitis damage index and the presence of chronic pulmonary or kidney disease. The risk of serious infection was higher in the rituximab group (relative risk (RR) 2.12, 95% CI 1.31-3.43).
Over 40% of patients with AAV experienced at least one SAE. Although shorter time to first SAE and higher risk of infection were observed in the rituximab group, baseline imbalances necessitate a careful interpretation of these results.
利妥昔单抗用于抗中性粒细胞胞浆抗体相关性血管炎(AAV)的诱导缓解及预防复发。本研究评估了安全性事件的发生率,并在现实环境中比较了利妥昔单抗队列与接受非利妥昔单抗治疗的队列发生首次严重不良事件(SAE)的时间。
血管炎利妥昔单抗监测研究是一项对2003年至2017年期间在一家专科血管炎诊所接受利妥昔单抗(美罗华)或其他治疗的AAV患者进行的回顾性观察研究。主要终点是发生首次SAE的时间。
共纳入392例患者:利妥昔单抗队列247例,对照组145例,总随访时间为2217人年(平均研究持续时间5.7年)。平均年龄为61岁,77%患有肉芽肿性多血管炎(GPA)。两组间基线特征(疾病持续时间和既往免疫抑制治疗使用情况)存在差异。利妥昔单抗组134/247例患者(54%)和对照组58/145例患者(40%)发生了至少一次SAE。利妥昔单抗组发生首次SAE的时间更短(风险比(HR)1.55,95%置信区间1.07 - 2.26,P = 0.022)。首次SAE的预测因素为较高的血管炎损伤指数以及慢性肺部或肾脏疾病的存在。利妥昔单抗组严重感染的风险更高(相对风险(RR)2.12,95%置信区间1.31 - 3.43)。
超过40%的AAV患者发生了至少一次SAE。尽管利妥昔单抗组观察到发生首次SAE的时间更短且感染风险更高,但基线不平衡使得对这些结果的解读需要谨慎。