Veldmeijer Lars, Terlouw Gijs, van Os Jim, Te Meerman Sanne, van 't Veer Job, Boonstra Nynke
Department of Psychiatry, Utrecht University Medical Center, Utrecht, Netherlands.
Digital Innovation in Health, NHL Stenden University of Applied Sciences, Leeuwarden, Netherlands.
Front Psychiatry. 2024 Aug 6;15:1426475. doi: 10.3389/fpsyt.2024.1426475. eCollection 2024.
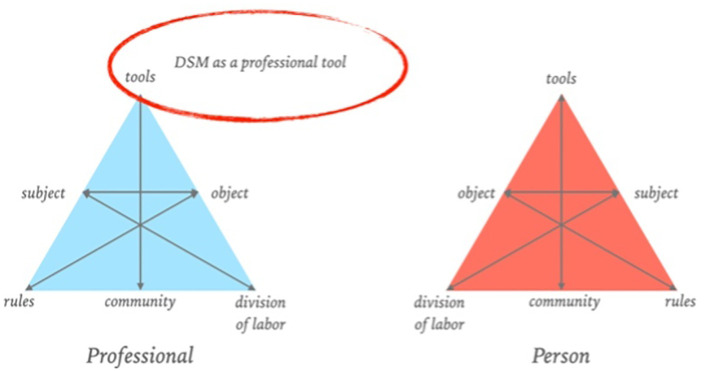
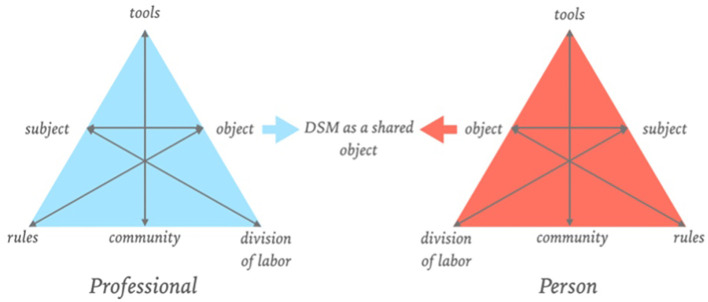
The Diagnostic and Statistical Manual of Mental Disorders, abbreviated as the DSM, is one of mental health care's most commonly used classification systems. While the DSM has been successful in establishing a shared language for researching and communicating about mental distress, it has its limitations as an empirical compass. In the transformation of mental health care towards a system that is centered around shared decision-making, person-centered care, and personal recovery, the DSM is problematic as it promotes the disengagement of people with mental distress and is primarily a tool developed for professionals to communicate patients instead of patients. However, the mental health care system is set up in such a way that we cannot do without the DSM for the time being. In this paper, we aimed to describe the position and role the DSM may have in a mental health care system that is evolving from a medical paradigm to a more self-contained profession in which there is increased accommodation of other perspectives. First, our analysis highlights the DSM's potential as a boundary object in clinical practice, that could support a shared language between patients and professionals. Using the DSM as a conversation piece, a language accommodating diverse perspectives can be co-created. Second, we delve into why people with lived experience should be involved in co-designing spectra of distress. We propose an iterative design and test approach for designing DSM spectra of distress in co-creation with people with lived experience to prevent the development of 'average solutions' for 'ordinary people'. We conclude that transforming mental health care by reconsidering the DSM as a boundary object and conversation piece between activity systems could be a step in the right direction, shifting the power balance towards shared ownership in a participation era that fosters dialogue instead of diagnosis.
《精神疾病诊断与统计手册》,简称为DSM,是心理健康护理领域最常用的分类系统之一。虽然DSM成功地建立了一种用于研究和交流心理困扰的共享语言,但作为一个实证指南,它有其局限性。在心理健康护理向以共同决策、以人为本的护理和个人康复为中心的系统转变过程中,DSM存在问题,因为它促使有心理困扰的人与护理脱节,并且主要是为专业人员开发的用于与患者沟通的工具,而非供患者使用。然而,心理健康护理系统的设置方式使我们目前离不开DSM。在本文中,我们旨在描述DSM在从医学范式向更具自主性的专业领域演变的心理健康护理系统中可能具有的地位和作用,在这个演变过程中,其他观点得到了更多的接纳。首先,我们的分析强调了DSM作为临床实践中的边界对象的潜力,它可以支持患者和专业人员之间的共享语言。将DSM用作话题,就可以共同创造一种包容不同观点的语言。其次,我们深入探讨了有实际生活经验的人为何应参与共同设计心理困扰谱。我们提出了一种迭代设计和测试方法,用于与有实际生活经验的人共同创建DSM心理困扰谱,以防止为“普通人”开发出“平均解决方案”。我们得出结论,通过将DSM重新视为活动系统之间的边界对象和话题来转变心理健康护理,可能是朝着正确方向迈出的一步,在一个促进对话而非诊断的参与时代,将权力平衡转向共享所有权。