Fassi Elena, Amoroso Vito, Cosentini Deborah, Ferrari Vittorio, Laganà Marta, Berruti Alfredo, di Mauro Pierluigi
Medical Oncology Unit, Department of Medical and Surgical Specialties, Radiological Sciences, and Public Health, University of Brescia. ASST Spedali Civili, Brescia, Italy.
Front Oncol. 2024 Aug 6;14:1398055. doi: 10.3389/fonc.2024.1398055. eCollection 2024.
Regorafenib is an oral multi-targeted tyrosine kinase inhibitor (TKI) indicated for the treatment of various tumor types, including metastatic gastrointestinal stromal tumors (GIST), as a third-line systemic therapy. Erythrocytosis, which is characterized by an increase in erythrocyte count, hemoglobin, and hematocrit levels, has been described as a side effect of some antiangiogenic TKIs but has never been associated with regorafenib administration.
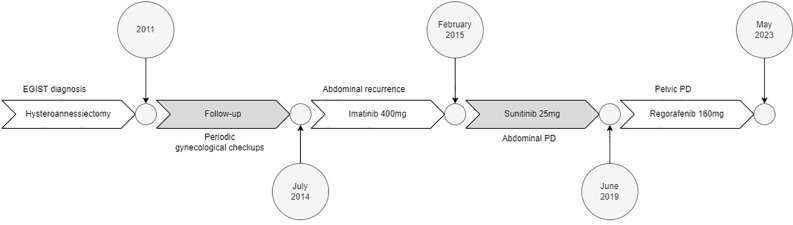
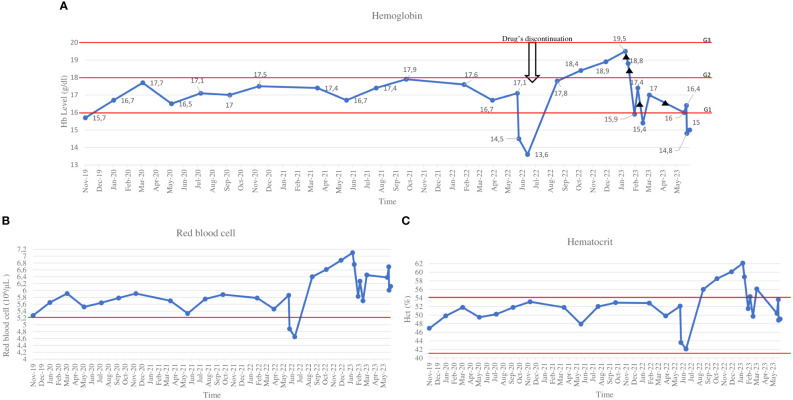
An extra-GIST was diagnosed in a 58-year-old woman after she underwent surgery to remove a pelvic mass. Three years later, systemic therapy with imatinib was started due to pelvic disease recurrence. However, after six months, due to disease progression, we prescribed sunitinib, which the patient received for four years. Regorafenib was initiated in June 2019, and after six months, we noted an increase in the erythrocytes' count and hemoglobin (Hb) levels. Given that the patient had clinical benefit and hematocrit was within normal range, we only monitored the blood cell count and continued to give regorafenib at the same dose. The drug was then stopped for over six weeks due to hospitalization for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, and Hb levels returned to normal. Therefore, we decided to restart regorafenib at a lower dose. However, Hb levels rose again in conjunction with increased hematocrit, resulting in the need for multiple phlebotomies. We attempted to restart regorafenib every other day, but it was unsuccessful, so we stopped it permanently in May 2023, and all values returned to normal.
Regorafenib may cause secondary erythrocytosis that could not be dose-related, as this case report suggests. Secondary erythrocytosis might be a marker of TKI efficacy, given the patient's prolonged clinical benefit during regorafenib treatment (48 months). In patients receiving regorafenib, monitoring blood count as well as any symptoms associated with erythrocytosis may be suggested.
瑞戈非尼是一种口服多靶点酪氨酸激酶抑制剂(TKI),被批准作为三线全身治疗药物用于治疗包括转移性胃肠道间质瘤(GIST)在内的多种肿瘤类型。红细胞增多症的特征是红细胞计数、血红蛋白和血细胞比容水平升高,已被描述为一些抗血管生成TKI的副作用,但从未与瑞戈非尼的使用相关联。
一名58岁女性在接受盆腔肿块切除手术后被诊断出患有非GIST肿瘤。三年后,由于盆腔疾病复发,开始使用伊马替尼进行全身治疗。然而,六个月后,由于疾病进展,我们开了舒尼替尼,患者接受了四年治疗。2019年6月开始使用瑞戈非尼,六个月后,我们注意到红细胞计数和血红蛋白(Hb)水平升高。鉴于患者有临床获益且血细胞比容在正常范围内,我们仅监测血细胞计数并继续以相同剂量给予瑞戈非尼。随后,由于感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)住院,该药物停用了六周多,Hb水平恢复正常。因此,我们决定以较低剂量重新开始使用瑞戈非尼。然而,Hb水平再次升高,同时血细胞比容增加,导致需要多次放血。我们试图每隔一天重新开始使用瑞戈非尼,但未成功,所以我们在2023年5月永久停用了它,所有指标恢复正常。
如本病例报告所示,瑞戈非尼可能会导致与剂量无关的继发性红细胞增多症。鉴于患者在瑞戈非尼治疗期间(48个月)有长期临床获益,继发性红细胞增多症可能是TKI疗效的一个标志。对于接受瑞戈非尼治疗的患者,建议监测血细胞计数以及与红细胞增多症相关的任何症状。