Department of Neurology, Minaminara General Medical Center, Yoshino, Nara, Japan.
Department of Neurology, Nara Medical University, Kashihara, Nara, Japan.
BMC Neurol. 2024 Aug 22;24(1):292. doi: 10.1186/s12883-024-03804-y.
Generalized myasthenia gravis (gMG) can be managed with acetylcholinesterase inhibitors (AChEis; e.g., pyridostigmine), corticosteroids, other immunosuppressive drugs (e.g., tacrolimus), and their combinations. Intravenous immunoglobulin (IVIg) or plasmapheresis (PLEX) may be administered if symptoms persist. PLEX and IVIg are also mainstays of treatment for myasthenic crisis. Recently, efgartigimod was approved in Japan for treating adults with gMG (irrespective of the antibody status) who do not have a sufficient response to corticosteroids and nonsteroidal immunosuppressive therapies. Efgartigimod is generally safe and well tolerated. However, since phase III trials of efgartigimod excluded those with myasthenic crisis, the efficacy of efgartigimod in treating myasthenic crisis is still unclear. Moreover, there are no reports that efgartigimod therapy can reduce the dose of corticosteroids needed to achieve a minimal manifestation status.
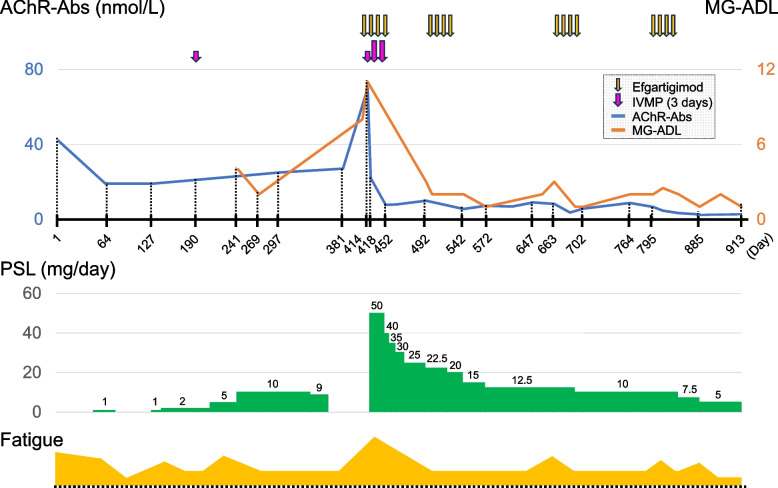
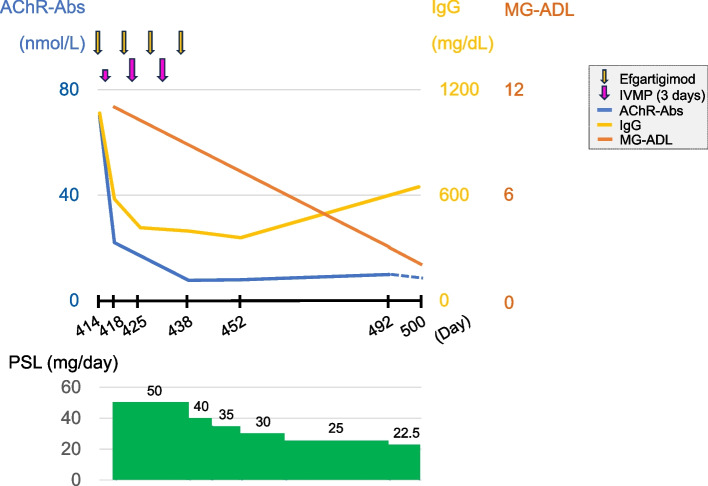
We report the case of a 70-yeat-old woman with gMG who developed a myasthenic crisis. After she was diagnosed with gMG, the patient had been treated with oral corticosteroids and tacrolimus for 1 year. However, she refused to continue taking the medication, and two weeks later, she developed ptosis, dysphagia and dyspnea. The patient was intubated and treated with efgartigimod in combination with steroid therapy, and she recovered without PLEX or IVIg. Afterward, when she experienced worsening of fatigue and increased levels of anti-acetylcholine receptor antibodies, efgartigimod therapy was effective. The patient achieved minimal manifestation status even after the reduction of corticosteroids and showed improvements in the Myasthenia Gravis Activities of Daily Living scales after 4 cycles of efgartigimod infusion.
Our case suggests that efgartigimod can be an alternative drug for achieving minimal manifestation status in patients with myasthenic crisis. Considering its strong efficacy and safety, efgartigimod could be expanded to use as bridging therapy in the acute and chronic phases of gMG.
全身性重症肌无力(gMG)可通过乙酰胆碱酯酶抑制剂(AChEis;例如吡啶斯的明)、皮质类固醇、其他免疫抑制剂(例如他克莫司)及其组合来治疗。如果症状持续存在,可能会给予静脉注射免疫球蛋白(IVIg)或血浆置换(PLEX)。PLEX 和 IVIg 也是治疗肌无力危象的主要方法。最近,依氟鸟氨酸在日本被批准用于治疗对皮质类固醇和非甾体免疫抑制剂治疗反应不足的 gMG 成年患者(无论抗体状态如何)。依氟鸟氨酸通常是安全且耐受良好的。然而,由于依氟鸟氨酸的 III 期试验排除了患有肌无力危象的患者,因此依氟鸟氨酸治疗肌无力危象的疗效仍不清楚。此外,尚无报告表明依氟鸟氨酸治疗可减少达到最小表现状态所需的皮质类固醇剂量。
我们报告了一例 70 岁女性 gMG 患者发生肌无力危象的病例。患者被诊断为 gMG 后,接受了口服皮质类固醇和他克莫司治疗 1 年。然而,她拒绝继续服药,两周后出现上睑下垂、吞咽困难和呼吸困难。患者被插管并接受依氟鸟氨酸联合类固醇治疗,未接受 PLEX 或 IVIg 治疗后康复。此后,当她出现疲劳加重和抗乙酰胆碱受体抗体水平升高时,依氟鸟氨酸治疗有效。即使在减少皮质类固醇后,患者仍达到最小表现状态,并在依氟鸟氨酸输注 4 个周期后在重症肌无力日常生活活动量表中得到改善。
我们的病例表明,依氟鸟氨酸可作为肌无力危象患者达到最小表现状态的替代药物。考虑到其强大的疗效和安全性,依氟鸟氨酸可扩展用于 gMG 的急性和慢性阶段的桥接治疗。