Ioannou Konstantinos, Bucci Marco, Tzortzakakis Antonios, Savitcheva Irina, Nordberg Agneta, Chiotis Konstantinos
Division of Clinical Geriatrics, Center for Alzheimer Research, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
Theme Inflammation and Aging, Karolinska University Hospital, Stockholm, Sweden.
Mol Psychiatry. 2025 Feb;30(2):587-599. doi: 10.1038/s41380-024-02672-9. Epub 2024 Aug 23.
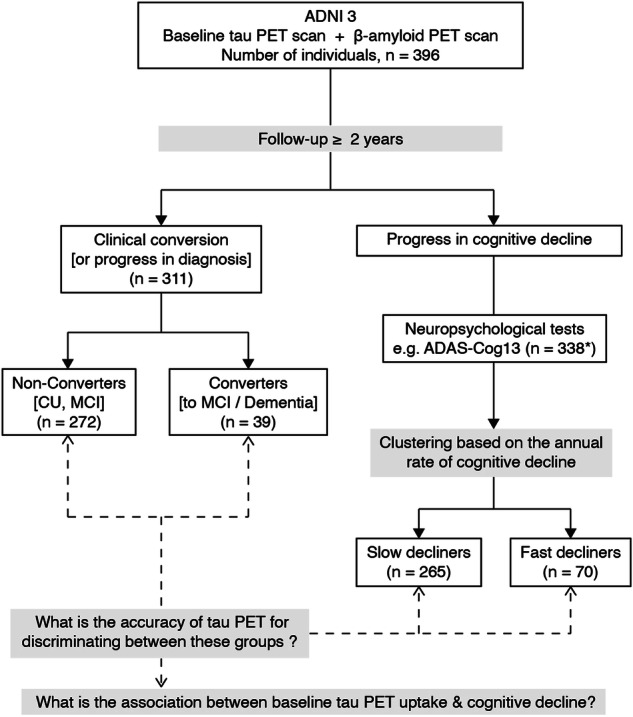
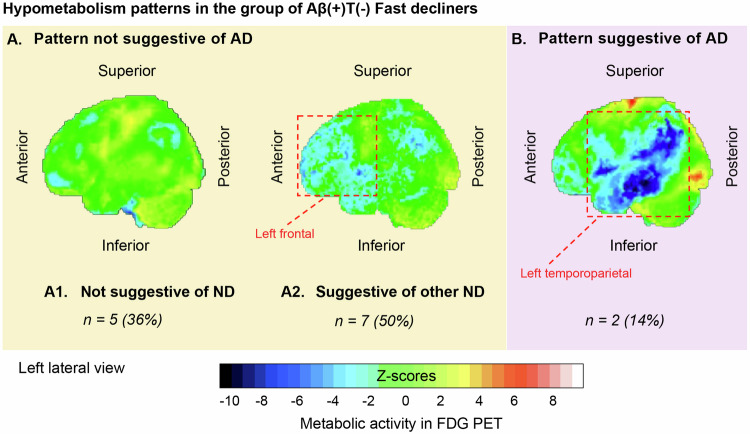
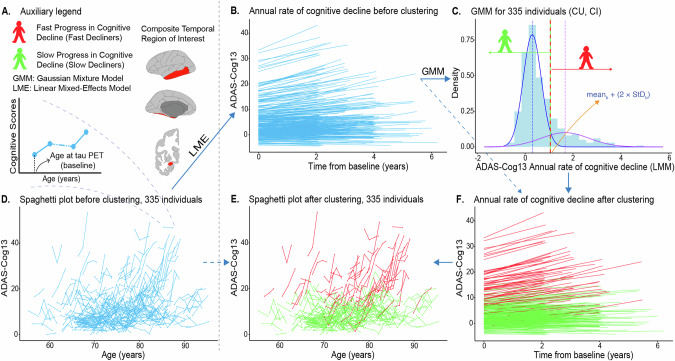
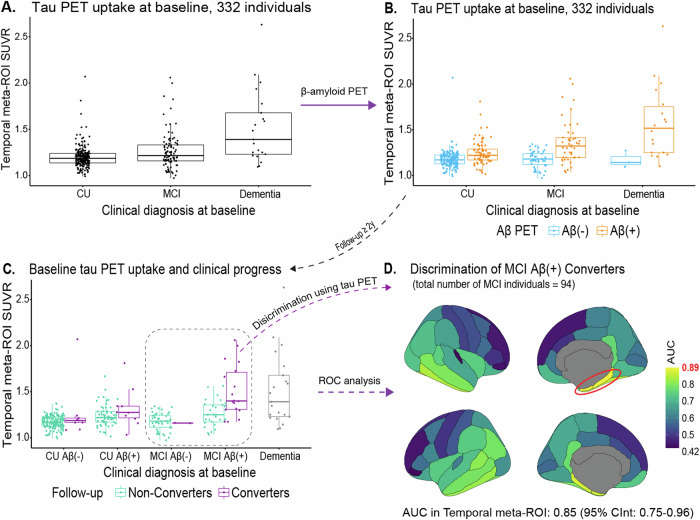
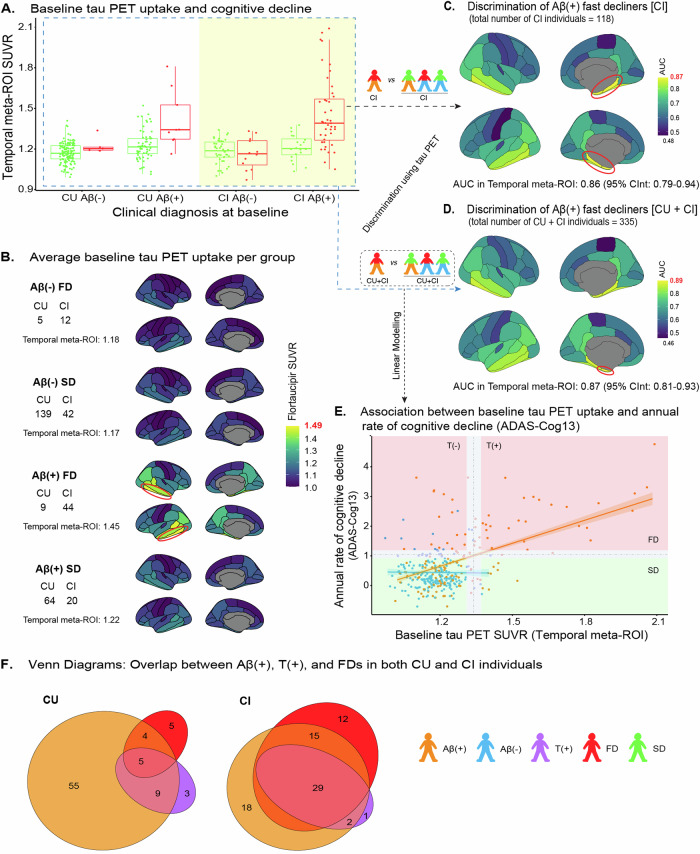
β-amyloid (Aβ) pathology is not always coupled with Alzheimer's disease (AD) relevant cognitive decline. We assessed the accuracy of tau PET to identify Aβ(+) individuals who show prospective disease progression. 396 cognitively unimpaired and impaired individuals with baseline Aβ and tau PET and a follow-up of ≥ 2 years were selected from the Alzheimer's Disease Neuroimaging Initiative dataset. The participants were dichotomously grouped based on either clinical conversion (i.e., change of diagnosis) or cognitive deterioration (fast (FDs) vs. slow decliners (SDs)) using data-driven clustering of the individual annual rates of cognitive decline. To assess cognitive decline in individuals with isolated Aβ(+) or absence of both Aβ and tau (T) pathologies, we investigated the prevalence of non-AD comorbidities and FDG PET hypometabolism patterns suggestive of AD. Baseline tau PET uptake was higher in Aβ(+)FDs than in Aβ(-)FD/SDs and Aβ(+)SDs, independently of baseline cognitive status. Baseline tau PET uptake identified MCI Aβ(+) Converters and Aβ(+)FDs with an area under the curve of 0.85 and 0.87 (composite temporal region of interest) respectively, and was linearly related to the annual rate of cognitive decline in Aβ(+) individuals. The T(+) individuals constituted largely a subgroup of those being Aβ(+) and those clustered as FDs. The most common biomarker profiles in FDs (n = 70) were Aβ(+)T(+) (n = 34, 49%) and Aβ(+)T(-) (n = 19, 27%). Baseline Aβ load was higher in Aβ(+)T(+)FDs (M = 83.03 ± 31.42CL) than in Aβ(+)T(-)FDs (M = 63.67 ± 26.75CL) (p-value = 0.038). Depression diagnosis was more prevalent in Aβ(+)T(-)FDs compared to Aβ(+)T(+)FDs (47% vs. 15%, p-value = 0.021), as were FDG PET hypometabolism pattern not suggestive of AD (86% vs. 50%, p-value = 0.039). Our findings suggest that high tau PET uptake is coupled with both Aβ pathology and accelerated cognitive decline. In cases of isolated Aβ(+), cognitive decline may be associated with changes within the AD spectrum in a multi-morbidity context, i.e., mixed AD.
β-淀粉样蛋白(Aβ)病理改变并不总是与阿尔茨海默病(AD)相关的认知功能下降相关联。我们评估了tau正电子发射断层扫描(PET)识别显示疾病进展的Aβ阳性个体的准确性。从阿尔茨海默病神经影像学倡议数据集选取了396名认知功能未受损和受损的个体,这些个体有基线Aβ和tau PET数据且随访时间≥2年。使用个体认知下降年率的数据驱动聚类,根据临床转化(即诊断变化)或认知恶化(快速衰退者(FDs)与缓慢衰退者(SDs))将参与者进行二分分组。为了评估孤立Aβ阳性或同时缺乏Aβ和tau(T)病理改变个体的认知下降情况,我们调查了非AD合并症的患病率以及提示AD的氟代脱氧葡萄糖(FDG)PET低代谢模式。无论基线认知状态如何,Aβ阳性FDs组的基线tau PET摄取高于Aβ阴性FD/SDs组和Aβ阳性SDs组。基线tau PET摄取分别以0.85和0.87的曲线下面积(复合颞叶感兴趣区)识别轻度认知障碍(MCI)Aβ阳性转化者和Aβ阳性FDs,并且与Aβ阳性个体的认知下降年率呈线性相关。T阳性个体主要构成Aβ阳性个体和聚类为FDs个体的一个亚组。FDs组(n = 70)中最常见的生物标志物谱为Aβ阳性T阳性(n = 34,49%)和Aβ阳性T阴性(n = 19,27%)。Aβ阳性T阳性FDs组的基线Aβ负荷(M = 83.03±31.42CL)高于Aβ阳性T阴性FDs组(M = 63.67±26.75CL)(p值 = 0.038)。与Aβ阳性T阳性FDs组相比,Aβ阳性T阴性FDs组中抑郁症诊断更为普遍(47%对15%,p值 = 0.021),提示非AD的FDG PET低代谢模式也是如此(86%对50%,p值 = 0.039)。我们的研究结果表明,高tau PET摄取与Aβ病理改变和加速的认知下降相关。在孤立Aβ阳性的情况下,认知下降可能与多病症背景下AD谱内的变化有关,即混合性AD。