Yango Jepsy, Tshomba Antoine Oloma, Kwete Papy, Madinga Joule, Mulangu Sabue, Mbala-Kingebeni Placide, Henriquez-Trujillo Aquiles R, Jacobs Bart K M
Department of Epidemiology and Global Health, Institut National de Recherche Biomédicale, Kinshasa, Democratic Republic of the Congo.
Department of Clinical Sciences, Institute of Tropical Medicine, Antwerp, Belgium.
PLOS Glob Public Health. 2024 Aug 26;4(8):e0003583. doi: 10.1371/journal.pgph.0003583. eCollection 2024.
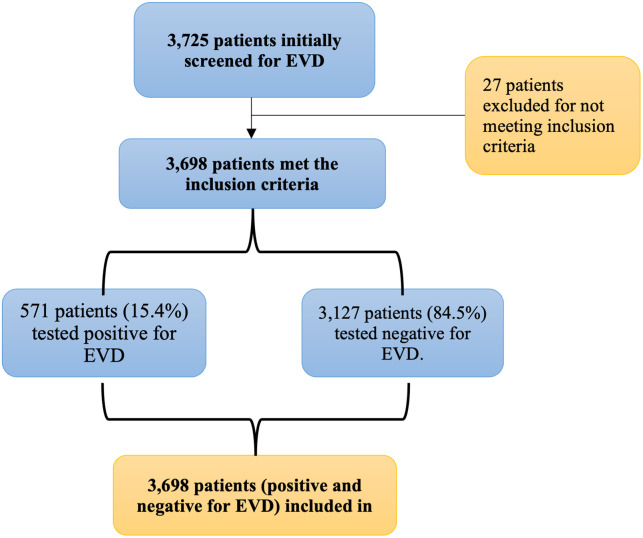
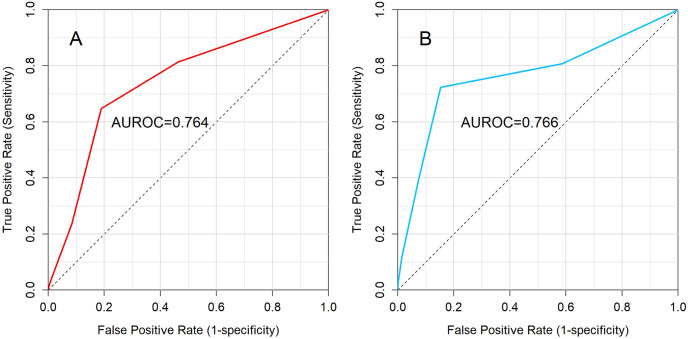
The 2018-2020 Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo (DRC) was the largest since the disease's discovery in 1976. Rapid identification and isolation of EVD patients are crucial during triage. This study aimed to develop a clinical prediction score for EVD using clinical and epidemiological predictors. We conducted a retrospective cross-sectional study using surveillance data from EVD outbreak, collected during routine clinical care at the Ebola Transit Center (ETC) in Beni, DRC, from 2018 to 2020. The Spiegelhalter and Knill-Jones method was used for score development, including potential predictors with an adjusted likelihood ratio above 2 or below 0.50. Validation was performed using a dataset previously published in PLOSOne by Tshomba et al. Among 3725 patients screened, 3698 fulfilled the inclusion criteria, with 571 (15.4%) testing positive for EVD via RT-PCR Test. Seven predictive factors were identified: asthenia, sore throat, conjunctivitis, bleeding gums, hematemesis, contact with a sick person, and contact with a traditional healer. The prediction score achieved an Area under the receiver operating characteristic (AUROC) of 0.764, with 81.4% sensitivity and 53.6% specificity at a -1 cutoff. External validation demonstrated an AUROC of 0.766, with 80.8% sensitivity and 41.4% specificity at the -1 cutoff. Our study developed a screening tool to assess the risk of suspected patients developing EVD and being admitted to ETUs for RT-PCR testing and treatment. External validation results affirmed the model's reliability and generalizability in similar settings, suggesting its potential integration into clinical practice. Given the severity and urgency of EVD as well as the risk nosocomial EVD transmission, it is essential to continuously update these models with real-time data on symptoms, disease progression, patient outcomes and validated RDT during EVD outbreaks. This approach will enhance model accuracy, enabling more precise risk assessments and more effective outbreak management.
2018 - 2020年刚果民主共和国爆发的埃博拉病毒病疫情是自1976年该疾病被发现以来规模最大的一次。在分诊过程中,快速识别和隔离埃博拉病毒病患者至关重要。本研究旨在利用临床和流行病学预测指标开发一种埃博拉病毒病的临床预测评分系统。我们进行了一项回顾性横断面研究,使用了2018年至2020年在刚果民主共和国贝尼的埃博拉转运中心(ETC)进行常规临床护理期间收集的埃博拉病毒病疫情监测数据。采用斯皮格尔哈特和尼尔 - 琼斯方法进行评分系统开发,纳入调整似然比高于2或低于0.50的潜在预测指标。使用Tshomba等人先前发表在《公共科学图书馆·综合》上的数据集进行验证。在3725名接受筛查的患者中,3698名符合纳入标准,其中571名(15.4%)通过逆转录聚合酶链反应(RT-PCR)检测确诊为埃博拉病毒病阳性。确定了七个预测因素:乏力、咽痛、结膜炎、牙龈出血、呕血、与病人接触以及与传统治疗师接触。该预测评分系统在受试者工作特征曲线下面积(AUROC)为0.764,在截断值为 -1时,灵敏度为81.4%,特异度为53.6%。外部验证显示,在截断值为 -1时,AUROC为0.766,灵敏度为80.8%,特异度为41.4%。我们的研究开发了一种筛查工具,用于评估疑似患者感染埃博拉病毒病并被收治到埃博拉治疗单元进行RT-PCR检测和治疗的风险。外部验证结果证实了该模型在类似环境中的可靠性和可推广性,表明其有可能整合到临床实践中。鉴于埃博拉病毒病的严重性和紧迫性以及医院内埃博拉病毒病传播的风险,在埃博拉病毒病疫情期间,利用症状、疾病进展、患者结局和经过验证的快速诊断检测的实时数据持续更新这些模型至关重要。这种方法将提高模型的准确性,实现更精确的风险评估和更有效的疫情管理。