Department of Nursing, Zhongshan Hospital, Fudan University, Shanghai, China.
Department of Cardiac Surgery Intensive Care Unit, Zhongshan Hospital, Fudan University, Shanghai, China.
BMC Anesthesiol. 2024 Aug 28;24(1):298. doi: 10.1186/s12871-024-02672-w.
Acute kidney injury (AKI) significantly increases morbidity and mortality following cardiac surgery, especially in patients with pre-existing renal impairments. N-terminal pro-B-type natriuretic peptide (NT-proBNP) is a marker of cardiac stress and dysfunction, conditions often exacerbated during cardiac surgery and prevalent in chronic kidney disease (CKD) patients. Elevated NT-proBNP levels can indicate underlying cardiac strain, hemodynamic instability and volume overload. This study evaluated the association between perioperative changes in NT-proBNP levels and the incidence of AKI in this particular patient group.
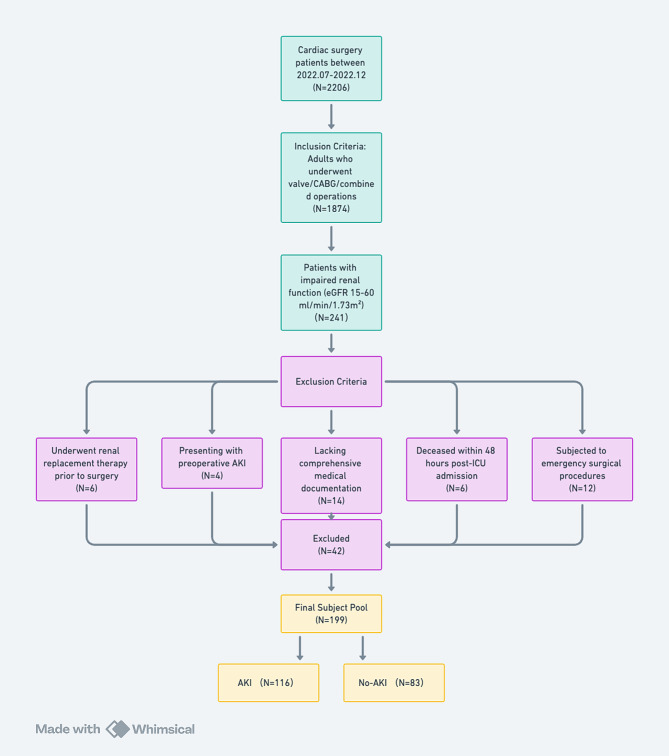
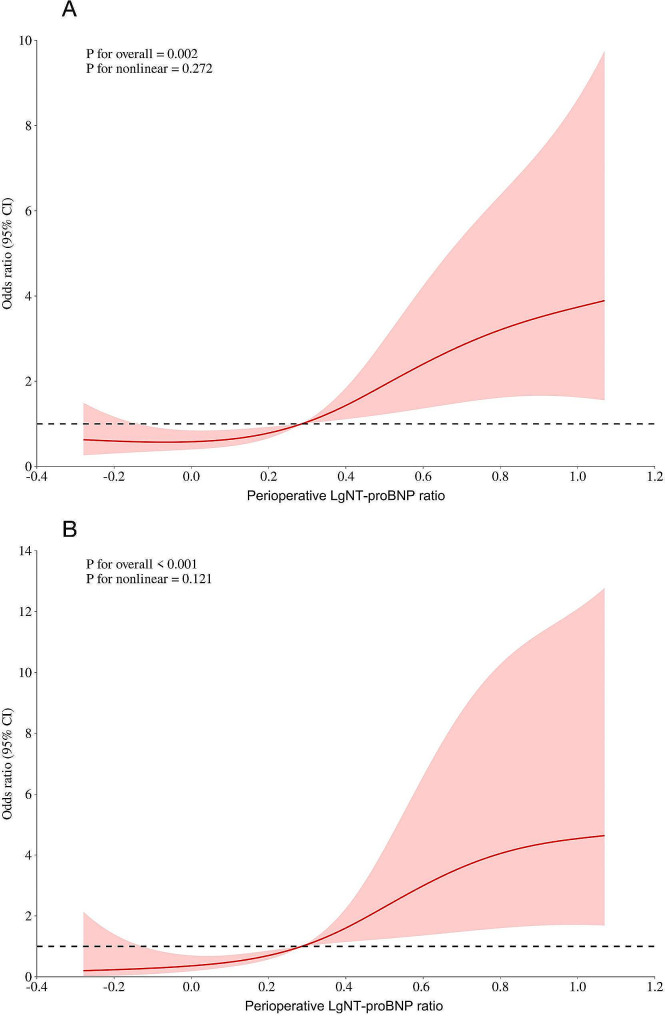
This retrospective study involved patients with impaired renal function (eGFR 15-60 ml/min/1.73 m²) who underwent cardiac surgery from July to December 2022. It analyzed the association between the ratio of preoperative and ICU admittance post-surgery NT-proBNP levels and the development of AKI and AKI stage 2-3, based on KDIGO criteria, using multivariate logistic regression models. Restricted cubic spline analysis assessed non-linear associations between NT-proBNP and endpoints. Subgroup analysis was performed to assess the heterogeneity of the association between NT-proBNP and endpoints in subgroups.
Among the 199 participants, 116 developed postoperative AKI and 16 required renal replacement therapy. Patients with AKI showed significantly higher postoperative NT-proBNP levels compared to those without AKI. Decreased baseline eGFR and increased post/preoperative NT-proBNP ratios were associated with higher AKI risk. Specifically, the highest quantile post/preoperative NT-proBNP ratio indicated an approximately seven-fold increase in AKI risk and a ninefold increase in AKI stage 2-3 risk compared to the lowest quantile. The area under the receiver operating characteristic curve for predicting AKI and AKI stage 2-3 using NT-proBNP were 0.63 and 0.71, respectively, demonstrating moderate accuracy. Subgroup analysis demonstrated that the positive association between endpoints and logarithmic transformed post/preoperative NT-proBNP levels was consistently robust in subgroup analyses stratified by age, sex, surgery, CPB application, hypertension, diabetes status and fluid balance.
Perioperative NT-proBNP level changes are predictive of postoperative AKI in patients with pre-existing renal deficiencies undergoing cardiac surgery, aiding in risk assessment and patient management.
急性肾损伤(AKI)显著增加心脏手术后的发病率和死亡率,尤其是在存在预先存在的肾功能损害的患者中。N 末端脑利钠肽前体(NT-proBNP)是心脏应激和功能障碍的标志物,这些情况在心脏手术期间经常加重,并且在慢性肾病(CKD)患者中很常见。升高的 NT-proBNP 水平可指示潜在的心脏压力、血流动力学不稳定和容量超负荷。本研究评估了围手术期 NT-proBNP 水平变化与该特定患者群体中 AKI 发生率之间的关联。
本回顾性研究纳入了 2022 年 7 月至 12 月期间接受心脏手术且肾功能受损(eGFR 15-60 ml/min/1.73 m²)的患者。它使用多元逻辑回归模型,根据 KDIGO 标准,分析了术前和 ICU 入院后 NT-proBNP 水平比值与 AKI 和 AKI 2-3 期发展之间的关联。受限三次样条分析评估了 NT-proBNP 与终点之间的非线性关联。进行亚组分析以评估 NT-proBNP 与亚组中终点之间关联的异质性。
在 199 名参与者中,有 116 名患者术后发生 AKI,16 名患者需要肾脏替代治疗。与无 AKI 患者相比,发生 AKI 的患者术后 NT-proBNP 水平显著升高。较低的基线 eGFR 和增加的术后/术前 NT-proBNP 比值与更高的 AKI 风险相关。具体来说,与最低定量相比,最高定量的术后/术前 NT-proBNP 比值表明 AKI 风险增加约七倍,AKI 2-3 期风险增加九倍。使用 NT-proBNP 预测 AKI 和 AKI 2-3 时,受试者工作特征曲线下面积分别为 0.63 和 0.71,表明准确性中等。亚组分析表明,在按年龄、性别、手术、体外循环应用、高血压、糖尿病状态和液体平衡分层的亚组分析中,终点与对数转换后的术后/术前 NT-proBNP 水平之间的正相关关系始终稳健。
在接受心脏手术的预先存在肾功能不足的患者中,围手术期 NT-proBNP 水平变化可预测术后 AKI,有助于风险评估和患者管理。