Lee Cha Len, Freeman Mark, Burak Kelly W, Moffat Gordon T, O'Donnell Conor D J, Ding Philip Q, Lyubetska Hanna, Meyers Brandon M, Gordon Vallerie, Kosyachkova Ekaterina, Bucur Roxana, Cheung Winson Y, Knox Jennifer J, Tam Vincent C
Princess Margaret Cancer Center, University of Toronto, Toronto, ON M5G1Z5, Canada.
Tom Baker Cancer Center, University of Calgary, Calgary, AB T2N4N2, Canada.
Cancers (Basel). 2024 Aug 19;16(16):2878. doi: 10.3390/cancers16162878.
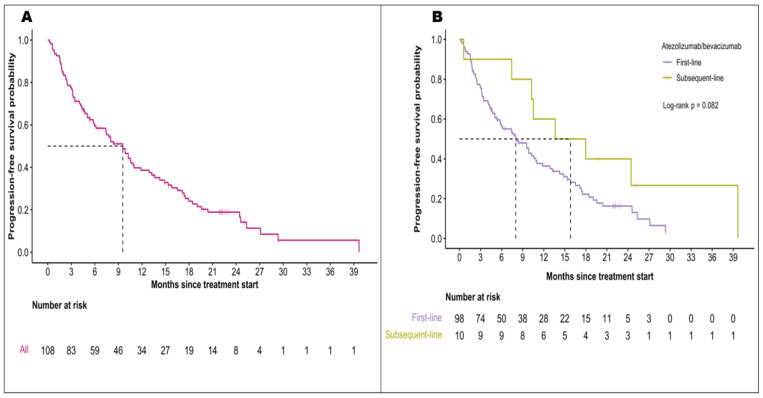
The IMbrave150 trial established atezolizumab with bevacizumab (A+B) as standard care for hepatocellular carcinoma (HCC), recommending an esophagogastroduodenoscopy (EGD) within 6 months of treatment initiation to prevent bleeding from esophagogastric varices. The necessity of mandatory EGD for all patients remains unclear. We retrospectively analyzed 112 HCC patients treated with A+B at five Canadian cancer centers from 1 July 2020 to 31 August 2022. A+B was the first-line therapy for 90% of patients, with median overall survival at 20.3 months and progression-free survival at 9.6 months. There was no survival difference between patients with bleeding and those without. Before A+B, 71% (n = 79) of patients underwent an EGD within 6 months, revealing varices in 41% (n = 32) and requiring intervention in 19% (n = 15). The overall bleeding rate was 15% (n = 17), with GI-specific bleeding occurring in 5% (n = 17). In the EGD group, GI-specific bleeding was 6% (n = 5) while in the non-EGD group, it was 3% (n = 1). Non-GI bleeding was observed in 10% (n = 11) of patients. Outcomes for HCC patients treated with A+B in Canada were comparable to IMbrave150. There was no increase in GI bleeding in patients without pre-treatment EGD, possibly supporting a selective EGD approach.
IMbrave150试验确立了阿替利珠单抗联合贝伐单抗(A+B)作为肝细胞癌(HCC)的标准治疗方案,并建议在开始治疗后的6个月内进行食管胃十二指肠镜检查(EGD),以预防食管胃静脉曲张出血。对于所有患者进行强制性EGD检查的必要性仍不明确。我们回顾性分析了2020年7月1日至2022年8月31日期间在加拿大五个癌症中心接受A+B治疗的112例HCC患者。A+B是90%患者的一线治疗方案,中位总生存期为20.3个月,无进展生存期为9.6个月。出血患者和未出血患者之间的生存率没有差异。在接受A+B治疗前,71%(n = 79)的患者在6个月内进行了EGD检查,其中41%(n = 32)发现有静脉曲张,19%(n = 15)需要干预。总体出血率为15%(n = 17),胃肠道特异性出血发生率为5%(n = 17)。在EGD检查组中,胃肠道特异性出血率为6%(n = 5),而在未进行EGD检查组中为3%(n = 1)。10%(n = 11)的患者出现非胃肠道出血。在加拿大接受A+B治疗的HCC患者的结果与IMbrave150试验相当。未进行治疗前EGD检查的患者胃肠道出血没有增加,这可能支持采用选择性EGD检查方法。