Graham David Y, Naser Saleh A, Borody Thomas, Hebzda Zbigniew, Sarles Harry, Levenson Scott, Hardi Robert, Arłukowicz Tomasz, Svorcan Petar, Fathi Reza, Bibliowicz Aida, Anderson Patricia, McLean Patrick, Fehrmann Clara, Harris M Scott, Zhao Shuhong, Kalfus Ira N
Departments of Medicine, Molecular Virology, and Microbiology, Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, TX 77030, USA.
Burnett School of Biomedical Sciences, University of Central Florida, Orlando, FL 32816, USA.
Antibiotics (Basel). 2024 Jul 25;13(8):694. doi: 10.3390/antibiotics13080694.
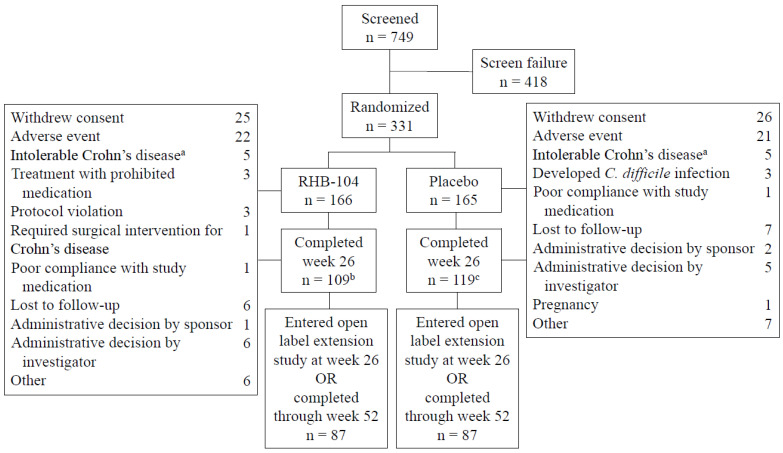
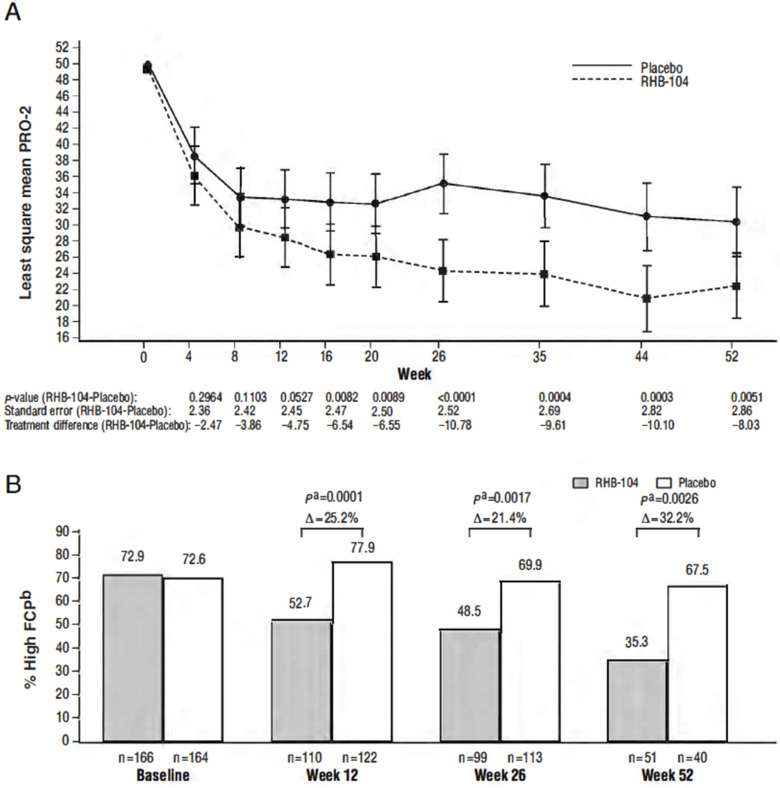
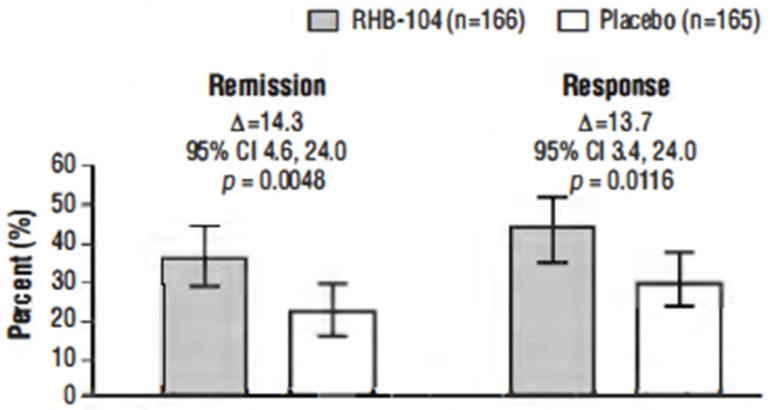
This study, conducted between 4 October 2013, and 30 November 2018, tested the hypothesis that triple antimicrobial therapy, targeting subspecies (MAP), long considered a putative cause, would favorably affect Crohn's disease. A double-blind multicenter study of adults with active Crohn's disease, (i.e., Crohn's Disease Activity Index [CDAI] 220-450 plus C-reactive protein ≥ 1.0 mg/dL, fecal calprotectin (FCP) >162.9 µg/g stool, or recent endoscopic or radiographic confirmation of active disease) receiving concomitant standard-of-care Crohn's disease treatment (Clinicaltrials.gov: NCT01951326) were stratified by anti-tumor necrosis factor use and randomized (1:1) to anti-MAP RHB-104 (clarithromycin 95 mg, rifabutin 45 mg, and clofazimine 10 mg per capsule) (n = 166), resulting in clarithromycin 950 mg/day, rifabutin 450 mg/day, and clofazimine 100 mg/day, or placebo (n = 165) for up to 52 weeks. A greater proportion of RHB-104 versus placebo-treated patients met the primary endpoint-remission (i.e., CDAI < 150)-at week 26 (36.7% [61/166] vs. 22.4% [37/165], respectively; 95% CI for difference: 4.6, 24.0, = 0.0048; chi-square test). Clinical response (reduction of CDAI by ≥100 points from baseline) at week 26 (first secondary endpoint) was also higher among the patients treated with RHB-104 (73/166 [44.0%]) compared with placebo (50/165 [30.3%]; 95% CI for difference: 3.4, 24.0, = 0.0116), and it remained higher at week 52 among the patients treated with RHB-104 (59/166 [35.5%] vs. (35/165 [21.2%] for placebo; 95% CI for difference: 4.7, 23.9, = 0.0042). A statistically significantly greater decline in FCP (another prospective efficacy endpoint) was also observed in RHB-104-treated patients, compared with placebo, at weeks 12, 26, and 52. The rates of serious adverse events were similar between groups (RHB-104: 18.7%; placebo: 18.8%). No patient died during the study. Antimicrobial therapy directed against MAP resulted in significantly greater improvement in clinical and laboratory (FCP) measures of active Crohn's disease.
本研究于2013年10月4日至2018年11月30日进行,检验了以下假设:针对长期以来被认为是可能病因的亚种(MAP)的三联抗菌疗法会对克罗恩病产生有利影响。一项针对成年活动性克罗恩病患者(即克罗恩病活动指数[CDAI]为220 - 450加上C反应蛋白≥1.0mg/dL、粪便钙卫蛋白(FCP)>162.9µg/g粪便,或近期内镜或影像学证实为活动性疾病)的双盲多中心研究,这些患者接受克罗恩病标准护理治疗(Clinicaltrials.gov:NCT01951326),根据抗肿瘤坏死因子的使用情况进行分层,并随机(1:1)分为抗MAP的RHB - 104组(每粒胶囊含克拉霉素95mg、利福布汀45mg和氯法齐明10mg)(n = 166),即每日服用克拉霉素950mg、利福布汀450mg和氯法齐明100mg,或安慰剂组(n = 165),治疗长达52周。在第26周时,与安慰剂治疗的患者相比,接受RHB - 104治疗的患者中有更大比例达到主要终点——缓解(即CDAI < 150)(分别为36.7%[61/166]对22.4%[37/165];差异的95%置信区间:4.6,24.0,P = 0.0048;卡方检验)。在第26周(第一个次要终点)时,接受RHB - 104治疗的患者的临床反应(CDAI较基线降低≥100分)也高于安慰剂组(73/166[44.0%]对50/165[30.3%];差异的95%置信区间:3.4,24.0,P = 0.0116),并且在第52周时,接受RHB - 104治疗的患者中该比例仍然更高(59/166[35.5%]对安慰剂组的35/165[21.2%];差异的95%置信区间:4.7,23.9,P = 0.0042)。在第12周、26周和52周时,与安慰剂相比,在接受RHB - 104治疗的患者中还观察到FCP(另一个前瞻性疗效终点)有统计学上显著更大幅度的下降。两组间严重不良事件发生率相似(RHB - 104组:18.7%;安慰剂组:18.8%)。研究期间无患者死亡。针对MAP的抗菌疗法在活动性克罗恩病患者的临床和实验室(FCP)指标方面带来了显著更大的改善。