Drobňaková Simona, Vargová Veronika, Barkai László
Department of Paediatrics and Adolescent Medicine, Faculty of Medicine, Pavol Jozef Šafárik University, 040 01 Kosice, Slovakia.
Physiological Controls Research Center, University Research and Innovation Center, Óbuda University, 1034 Budapest, Hungary.
Children (Basel). 2024 Jul 26;11(8):904. doi: 10.3390/children11080904.
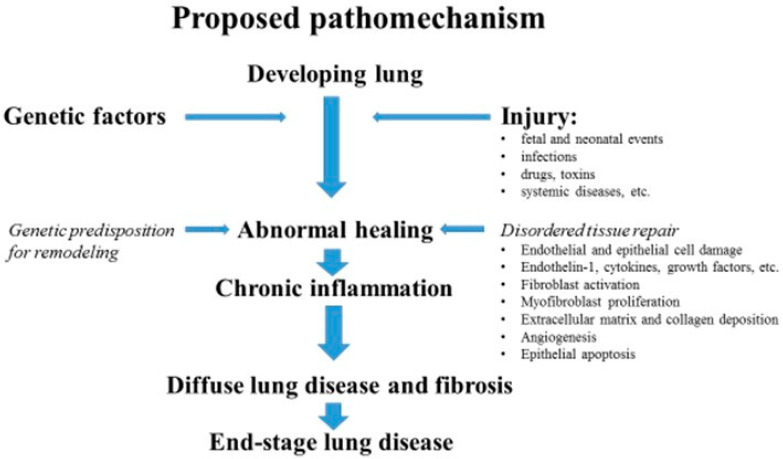
Interstitial lung disease (ILD) comprises a group of respiratory diseases affecting the interstitium of the lungs, which occur when a lung injury triggers an abnormal healing response, and an inflammatory process leads to altered diffusion and restrictive respiratory dysfunction. The term "interstitial" may be misleading, as other components of the lungs are usually also involved (epithelium, airways, endothelium, and so on). Pediatric conditions (childhood interstitial lung disease, chILD) are different from adult forms, as growing and developing lungs are affected and more diverse and less prevalent diseases are seen in childhood. Diffuse parenchymal lung disease (DPLD) and diffuse lung disease (DLD) can be used interchangeably with ILD. Known etiologies of chILD include chronic infections, bronchopulmonary dysplasia, aspiration, genetic mutations leading to surfactant dysfunction, and hypersensitivity pneumonitis due to drugs or environmental exposures. Many forms are seen in disorders with pulmonary involvement (connective tissue disorders, storage diseases, malignancies, and so on), but several conditions have unknown origins (desquamative pneumonitis, pulmonary interstitial glycogenosis, neuroendocrine cell hyperplasia in infancy, and so on). Currently, there is no consensus on pediatric classification; however, age grouping is proposed as some specific forms are more prevalent in infancy (developmental and growth abnormalities, surfactant dysfunction mutations, etc.) and others are usually seen in older cohorts (disorders in normal or immunocompromised hosts, systemic diseases, etc.). Clinical manifestations vary from mild nonspecific symptoms (recurrent respiratory infections, exercise intolerance, failure to thrive, dry cough, etc.) to a severe clinical picture (respiratory distress) and presentation related to the child's age. The diagnostic approach relies on imaging techniques (CT), but further investigations including genetic tests, BAL, and lung biopsy (VATS) are needed in uncertain cases. Pharmacological treatment is mostly empiric and based on anti-inflammatory and immunomodulatory drugs. Lung transplantation for selected cases in a pediatric transplantation center could be an option; however, limited data and evidence are available regarding long-term survival. International collaboration is warranted to understand chILD entities better and improve the outcomes of these patients.
间质性肺疾病(ILD)是一组影响肺间质的呼吸系统疾病,当肺损伤引发异常愈合反应且炎症过程导致弥散改变和限制性呼吸功能障碍时就会发生。“间质”一词可能会产生误导,因为肺的其他成分(上皮、气道、内皮等)通常也会受累。儿科疾病(儿童间质性肺疾病,chILD)与成人形式不同,因为生长发育中的肺会受到影响,儿童期可见更多样化且不太常见的疾病。弥漫性实质性肺疾病(DPLD)和弥漫性肺疾病(DLD)可与ILD互换使用。chILD的已知病因包括慢性感染、支气管肺发育不良、误吸、导致表面活性物质功能障碍的基因突变以及药物或环境暴露引起的过敏性肺炎。许多形式见于伴有肺部受累的疾病(结缔组织病、贮积病、恶性肿瘤等),但有几种情况病因不明(脱屑性肺炎、肺间质糖原沉积症、婴儿期神经内分泌细胞增生等)。目前,儿科分类尚无共识;然而,由于某些特定形式在婴儿期更常见(发育和生长异常、表面活性物质功能障碍突变等),而其他形式通常见于年龄较大的人群(正常或免疫功能低下宿主的疾病、全身性疾病等),因此建议进行年龄分组。临床表现从轻微的非特异性症状(反复呼吸道感染、运动不耐受、生长发育不良、干咳等)到严重的临床表现(呼吸窘迫)以及与儿童年龄相关的表现不等。诊断方法依赖于成像技术(CT),但在不确定的情况下需要进一步检查,包括基因检测、支气管肺泡灌洗(BAL)和肺活检(电视辅助胸腔镜手术,VATS)。药物治疗大多是经验性的,基于抗炎和免疫调节药物。在儿科移植中心,为选定病例进行肺移植可能是一种选择;然而,关于长期生存的可用数据和证据有限。有必要开展国际合作,以更好地了解chILD实体并改善这些患者的治疗效果。