Choi Hoon, Huh Jaewon, Kim Minju, Moon Seok Whan, Kim Kyung Soo, Hwang Wonjung
Department of Anesthesiology and Pain Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Republic of Korea.
Department of Thoracic and Cardiovascular Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Republic of Korea.
J Pers Med. 2024 Aug 21;14(8):881. doi: 10.3390/jpm14080881.
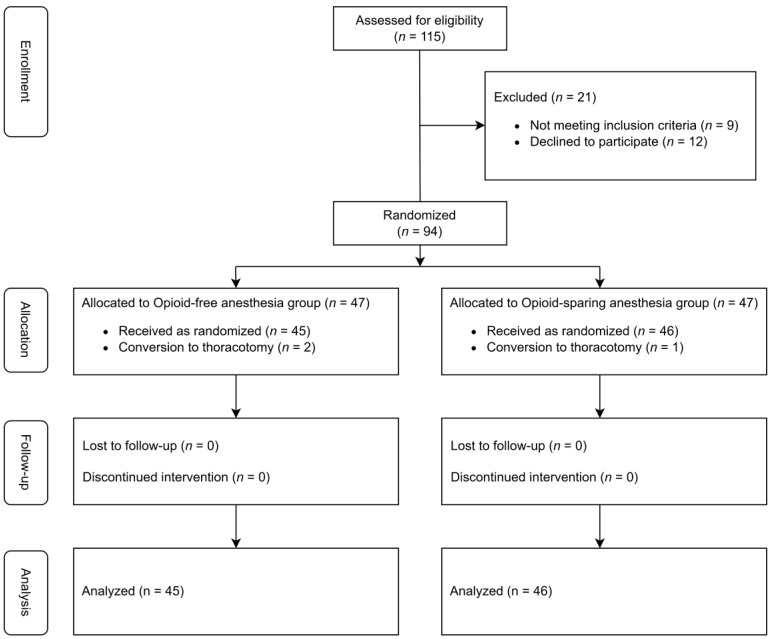
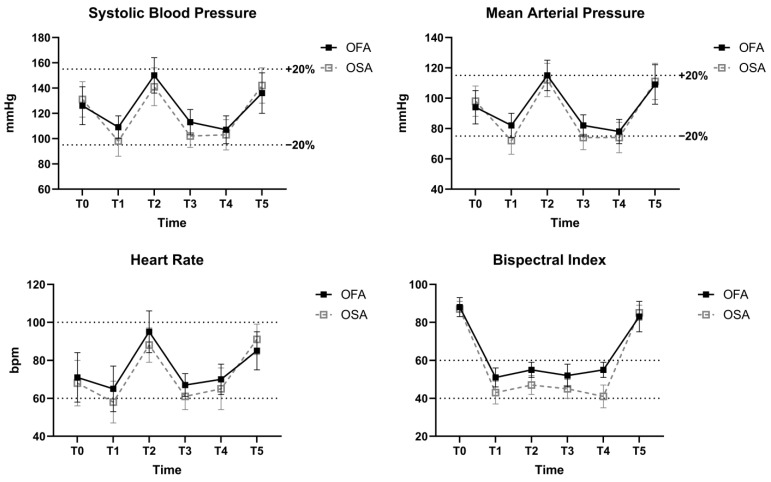
Opioids effectively manage perioperative pain but have numerous adverse effects. Opioid-free anesthesia (OFA) eliminates intraoperative opioid use; however, evidence for its use in video-assisted thoracoscopic surgery (VATS) is limited. This study assessed the effect of OFA using ketamine in VATS patients compared to opioid-sparing anesthesia (OSA). A total of 91 patients undergoing VATS lobectomy or segmentectomy were randomized to either the OFA group (ketamine) or the OSA group (remifentanil). The primary outcome was the quality of recovery (QoR) on postoperative day (POD) 1, measured with the QoR-40 questionnaire. Secondary outcomes included postoperative pain scores and adverse events. Both groups had comparable baseline and surgical characteristics. On POD 1, the QoR-40 score was higher in the OFA group than in the OSA group (164.3 ± 10.8 vs. 158.7 ± 10.6; mean difference: 5.6, 95% CI: 1.1, 10.0; = 0.015), though this did not meet the pre-specified minimal clinically important difference of 6.3. The visual analog scale score was lower in the OFA group as compared to the OSA group at 0-1 h (4.2 ± 2.3 vs. 6.2 ± 2.1; < 0.001) and 1-4 h after surgery (3.4 ± 1.8 vs. 4.6 ± 1.9; = 0.003). The OFA group had a lower incidence of PONV (2 [4.4%] vs. 9 [19.6%]; = 0.049) and postoperative shivering (4 [8.9%] vs. 13 [28.3%]; = 0.030) than the OSA group at 0-1 h after surgery. Using OFA with ketamine proved feasible, as indicated by the stable intraoperative hemodynamics and absence of intraoperative awareness. Patients undergoing VATS with OFA using ketamine showed a statistically significant, but clinically insignificant, QoR improvement compared to those receiving OSA with remifentanil.
阿片类药物能有效控制围手术期疼痛,但有诸多不良反应。无阿片类药物麻醉(OFA)可消除术中阿片类药物的使用;然而,其在电视辅助胸腔镜手术(VATS)中应用的证据有限。本研究评估了与保留阿片类药物麻醉(OSA)相比,在VATS患者中使用氯胺酮进行OFA的效果。总共91例行VATS肺叶切除术或肺段切除术的患者被随机分为OFA组(氯胺酮)或OSA组(瑞芬太尼)。主要结局是术后第1天(POD 1)的恢复质量(QoR),采用QoR - 40问卷进行测量。次要结局包括术后疼痛评分和不良事件。两组的基线和手术特征具有可比性。在POD 1时,OFA组的QoR - 40评分高于OSA组(164.3±10.8 vs. 158.7±10.6;平均差值:5.6,95%CI:1.1,10.0;P = 0.015),尽管这未达到预先设定的最小临床重要差异6.3。与OSA组相比,OFA组在术后0 - 1小时(4.2±2.3 vs. 6.2±2.1;P < 0.001)和术后1 - 4小时(3.4±1.8 vs. 4.6±1.9;P = 0.003)的视觉模拟量表评分更低。在术后0 - 1小时,OFA组恶心呕吐(PONV)的发生率低于OSA组(2 [4.4%] vs. 9 [19.6%];P = 0.049),术后寒战的发生率也低于OSA组(4 [8.9%] vs. 13 [28.3%];P = 0.030)。术中血流动力学稳定且未出现术中知晓,表明使用氯胺酮进行OFA是可行的。与接受瑞芬太尼OSA的患者相比,使用氯胺酮进行OFA的VATS患者在QoR方面有统计学上的显著改善,但临床意义不显著。